

Nasopharyngeal aspirates in children with severe community-acquired pneumonia collected within 3 days before bronchoscopy can partially reflect the pathogens in bronchoalveolar lavage fluids
- PMID: 36319953
- PMCID: PMC9623994
- DOI: 10.1186/s12879-022-07749-w
Nasopharyngeal aspirates in children with severe community-acquired pneumonia collected within 3 days before bronchoscopy can partially reflect the pathogens in bronchoalveolar lavage fluids
Abstract
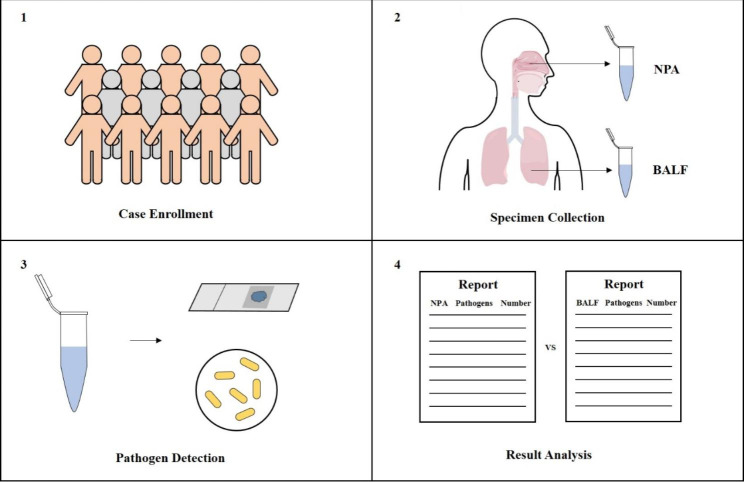
Background: There is little evidence about consistency between nasopharyngeal and pulmonary pathogens in children with severe pneumonia. This study aims to compare the difference of pathogens between nasopharyngeal aspirates (NPAs) collected before bronchoscopy and bronchoalveolar lavage fluids (BALFs) in children with severe community-acquired pneumonia (SCAP).
Methods: NPAs and BALFs were collected form pediatric SCAP cases hospitalized from January 2018 to March 2019. NPAs were colleced within 3 days before bronchoscopy. Samples were detected by direct immunofluorescence assay (DFA) for seven respiratory viruses and by routine bacterial culture in the clinical microbiology laboratory. Respiratory syncytial virus (RSV), Adenovirus (ADV), Influenza virus types A, B (IV-A and IV-B), Parainfluenza virus 1-3 (PIV1-3) were detected with a commercial assay. The virological and bacteriological detention results of NPAs were compared with the results of BALFs.
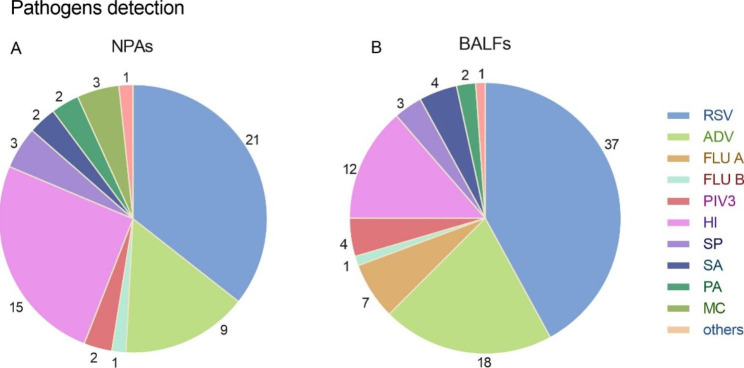
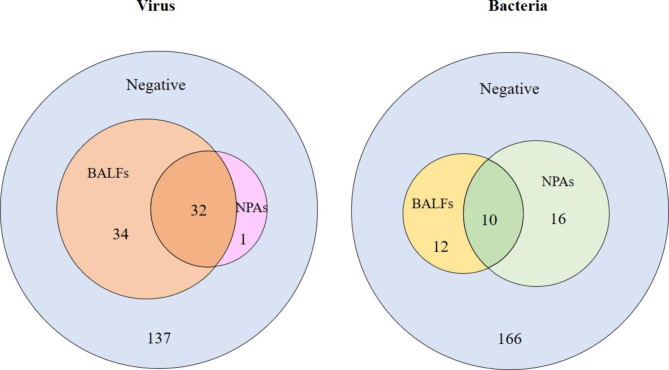
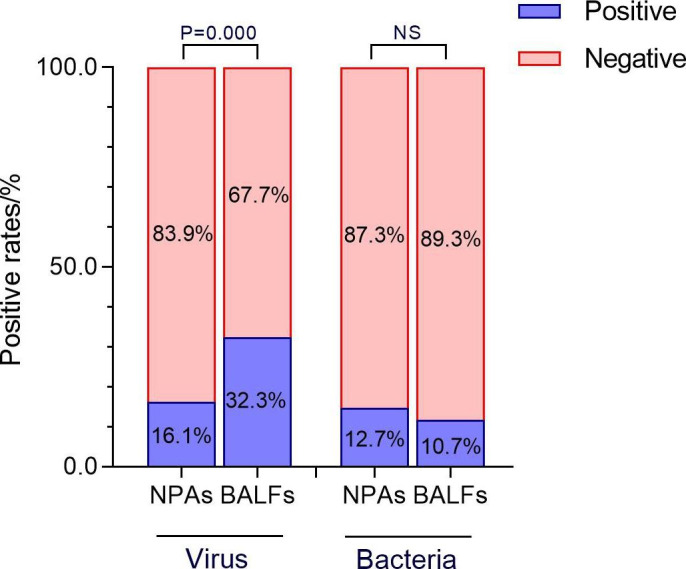
Results: In total 204 cases with mean age of 3.4 ± 2.8 years (IQR, 1 month-14 years) were included in the study. Both NPA and BALF were collected from those cases. The positive rates of pathogen in NPAs and BALFs were 25.0% (51/204) and 36.7% (75/204), respectively (x2 = 6.614, P = 0.010). Respiratory viruses were found in 16.1% (33/204) from NPAs and 32.3% (66/204) from BALFs (x2 = 14.524, P < 0.001). RSV and ADV were the two most frequent detected viruses in NPAs and BALFs. High consistentcy of pathogens between NPAs and BALFs was observed, and 96.9% (32/33) viruses detected in NPAs were also found in BALFs. While bacteria were isolated from 12.7% (26/204) and 10.7% (22/204) of the two kinds of samples, respectively (x2 = 0.378, P = 0.539). In addition, Haemophilus influenzae (HI) was the dominant germ in both samples.
Conclusion: The DFA method used to detect seven respiratory viruses from NPAs collected within 3 days before bronchoscopy can partially reflect the pathogens in the lungs in children with SCAP.
Keywords: Bronchoalveolar lavage fluid; Children; Etiology; Nasopharyngeal aspirate; Severe community-acquired pneumonia.
© 2022. The Author(s).
Conflict of interest statement
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Diagnostic Value of Nasopharyngeal Aspirates in Children with Lower Respiratory Tract Infections.Chin Med J (Engl). 2017 Mar 20;130(6):647-651. doi: 10.4103/0366-6999.201595. Chin Med J (Engl). 2017. PMID: 28303845 Free PMC article.
-
Mycoplasma pneumoniae and Adenovirus Coinfection Cause Pediatric Severe Community-Acquired Pneumonia.Microbiol Spectr. 2022 Apr 27;10(2):e0002622. doi: 10.1128/spectrum.00026-22. Epub 2022 Mar 21. Microbiol Spectr. 2022. PMID: 35311565 Free PMC article.
-
Interpretation of pathogenicity and clinical features of multiple pathogens in pediatric lower respiratory tract infections by tNGS RPTM analysis.Eur J Clin Microbiol Infect Dis. 2025 Jun;44(6):1313-1324. doi: 10.1007/s10096-025-05094-9. Epub 2025 Mar 14. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40085381
-
Clinical characteristics of severe community-acquired pneumonia in children with virus mono-detection versus co-detection with bacteria.BMC Pulm Med. 2025 Mar 21;25(1):130. doi: 10.1186/s12890-025-03591-3. BMC Pulm Med. 2025. PMID: 40119295 Free PMC article.
-
Epidemiology and Diagnostic Accuracy of Respiratory Pathogens in Pediatric Populations: Insights From Global Studies.Cureus. 2024 Sep 4;16(9):e68652. doi: 10.7759/cureus.68652. eCollection 2024 Sep. Cureus. 2024. PMID: 39371774 Free PMC article. Review.
Cited by
-
Clinical characteristics of pediatric patients hospitalized with community-acquired pneumonia and cytomegalovirus DNA detected in bronchoalveolar lavage fluid.Front Pediatr. 2024 Jul 24;12:1407174. doi: 10.3389/fped.2024.1407174. eCollection 2024. Front Pediatr. 2024. PMID: 39114856 Free PMC article.
-
Comparison of Real-time Polymerase Chain Reaction and Culture for Targeting Pathogens in Pediatric Severe Community-Acquired Pneumonia.Turk Arch Pediatr. 2024 Jul 1;59(4):383-389. doi: 10.5152/TurkArchPediatr.2024.24005. Turk Arch Pediatr. 2024. PMID: 39450793 Free PMC article.
-
Dynamics of platelet parameters in children with severe community-acquired pneumonia between viral and bacterial infections.Transl Pediatr. 2024 Jan 29;13(1):52-62. doi: 10.21037/tp-23-441. Epub 2024 Jan 18. Transl Pediatr. 2024. PMID: 38323174 Free PMC article.
-
Adenovirus and Mycoplasma pneumoniae co-infection as a risk factor for severe community-acquired pneumonia in children.Front Pediatr. 2024 Jan 31;12:1337786. doi: 10.3389/fped.2024.1337786. eCollection 2024. Front Pediatr. 2024. PMID: 38357505 Free PMC article.
-
Application of Targeted Next-Generation Sequencing in Bronchoalveolar Lavage Fluid for the Detection of Pathogens in Pulmonary Infections.Infect Drug Resist. 2025 Jan 27;18:511-522. doi: 10.2147/IDR.S499265. eCollection 2025. Infect Drug Resist. 2025. PMID: 39898354 Free PMC article.
References
-
- Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–35. doi: 10.1016/S0140-6736(16)31593-8. - DOI - PMC - PubMed
-
- Nair H, Simões EA, Rudan I, Gessner BD, Azziz-Baumgartner E, Zhang JSF, et al. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet. 2013;381(9875):1380–90. doi: 10.1016/S0140-6736(12)61901-1. - DOI - PMC - PubMed
-
- Miller JM, Binnicker MJ, Campbell S, Carroll KC, Chapin KC, Gilligan PH, et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clin Infect Dis. 2018;67(6):e1–94. doi: 10.1093/cid/ciy381. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
