

Waist-hip ratio measured by bioelectrical impedance analysis as a valuable predictor of chronic kidney disease development
- PMID: 36319963
- PMCID: PMC9623989
- DOI: 10.1186/s12882-022-02981-7
Waist-hip ratio measured by bioelectrical impedance analysis as a valuable predictor of chronic kidney disease development
Abstract
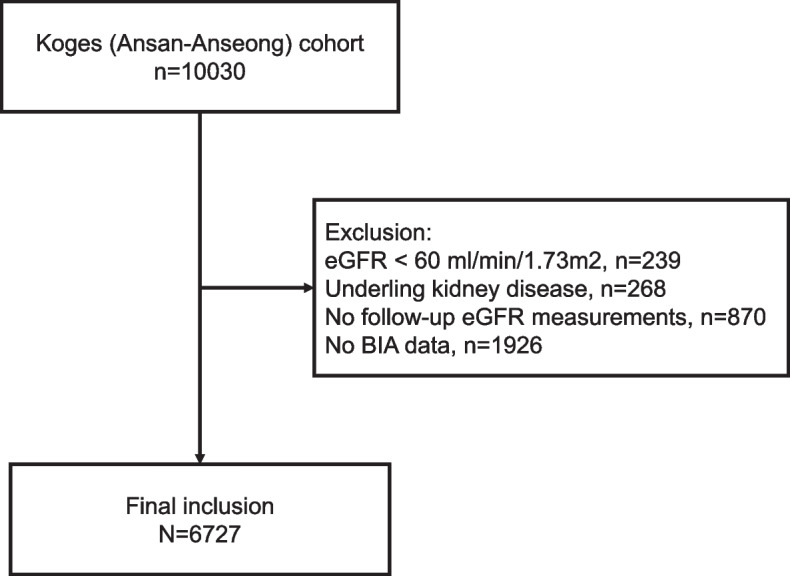
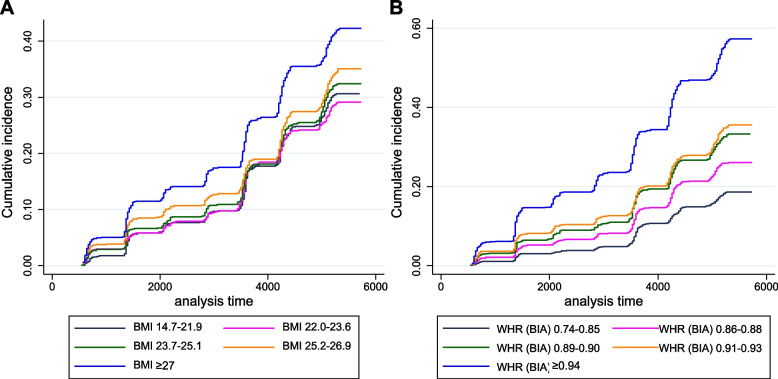
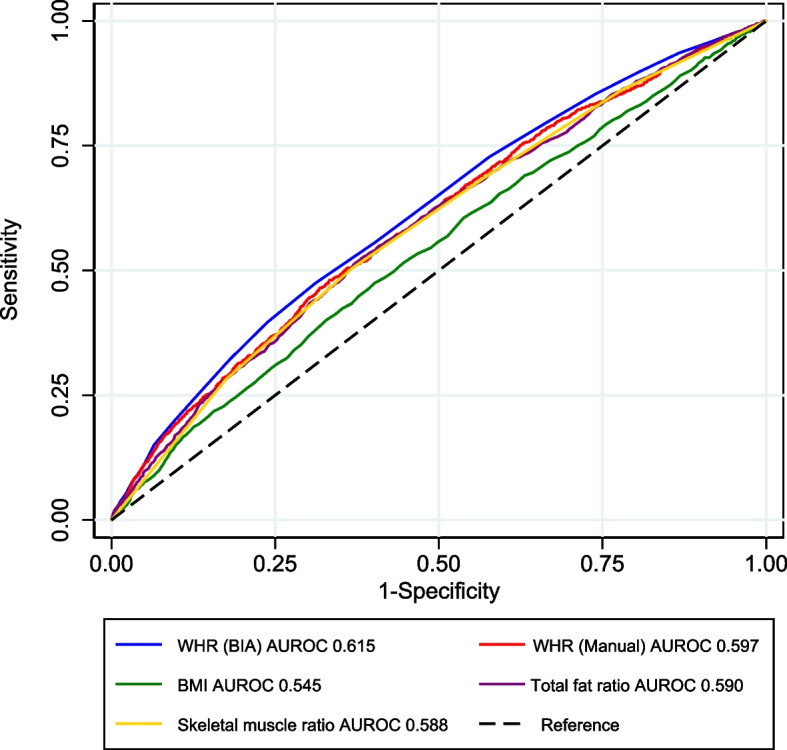
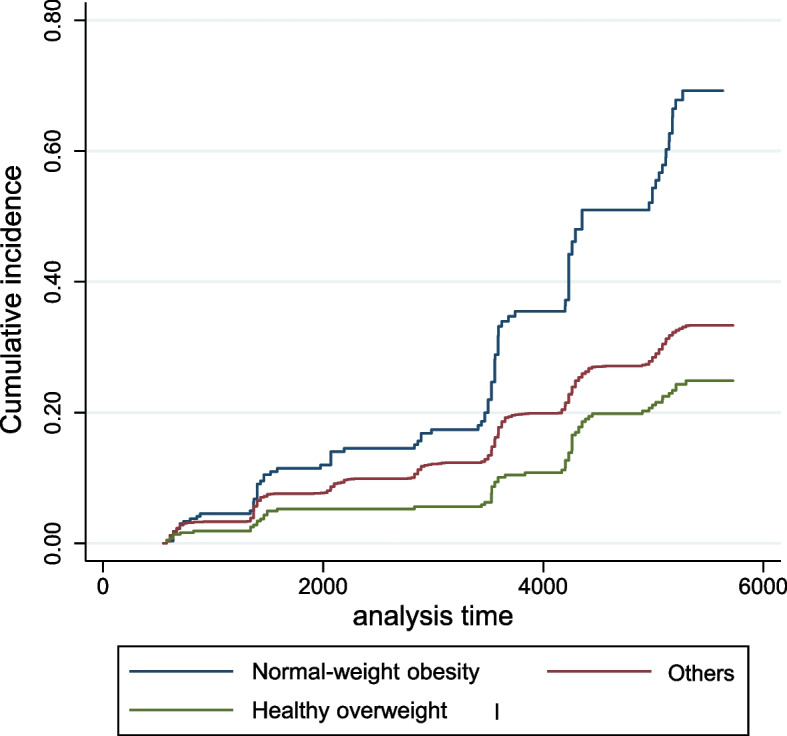
Obesity is a major health problem worldwide and is associated with chronic kidney disease (CKD). Body mass index (BMI) is a common method of diagnosing obesity, but there are concerns about its accuracy and ability to measure body composition. This study evaluated the risk of CKD development in a middle-aged population in association with various body composition metrics. From a prospective cohort of 10,030 middle-aged adults, we enrolled 6727 for whom baseline and follow-up data were available. We collected data pertaining to participants' BMI, manually measured waist-hip ratio (WHR), and various measurements of bioelectrical impedance analysis (BIA), including total body fat content, muscle content, and calculated WHR, and classified the participants into quintiles accordingly. CKD was defined as an estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73 m2 in follow-up laboratory tests. While an increase in BMI, WHR, and total body fat were associated with an elevated risk of CKD, an increase in total body muscle decreased the risk. Among the body composition metrics, WHR measured by BIA had the highest predictive value for CKD (C-statistics: 0.615). In addition, participants who were "healthy overweight, (defined as low WHR but high BMI), exhibited a 62% lower risk of developing CKD compared to those with "normal-weight obesity," (defined as high WHR despite a normal BMI). In conclusion, we suggest that central obesity measured by BIA is a more accurate indicator than BMI for predicting the development of CKD.
Keywords: Bioelectrical impedance analysis; Body mass index; Chronic kidney disease; Obesity.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Comparison of overall obesity and abdominal adiposity in predicting chronic kidney disease incidence among adults.J Ren Nutr. 2009 May;19(3):228-37. doi: 10.1053/j.jrn.2008.11.005. Epub 2009 Mar 3. J Ren Nutr. 2009. PMID: 19261489
-
Waist-to-hip ratio and body mass index as risk factors for cardiovascular events in CKD.Am J Kidney Dis. 2008 Jul;52(1):49-57. doi: 10.1053/j.ajkd.2008.04.002. Epub 2008 Jun 2. Am J Kidney Dis. 2008. PMID: 18514990 Free PMC article.
-
Body mass index combined with waist circumference can predict moderate chronic kidney disease: A retrospective study.Medicine (Baltimore). 2021 Mar 26;100(12):e25017. doi: 10.1097/MD.0000000000025017. Medicine (Baltimore). 2021. PMID: 33761657 Free PMC article.
-
Assessment of obesity in chronic kidney disease: what is the best measure?Curr Opin Nephrol Hypertens. 2012 Nov;21(6):641-6. doi: 10.1097/MNH.0b013e328358a02b. Curr Opin Nephrol Hypertens. 2012. PMID: 23010758 Review.
-
Exploring obesity phenotypes: a longitudinal perspective.Rev Endocr Metab Disord. 2025 Jun 18. doi: 10.1007/s11154-025-09976-3. Online ahead of print. Rev Endocr Metab Disord. 2025. PMID: 40528138 Review.
Cited by
-
Association between abdominal fat distribution and urinary albumin/creatinine ratio in patients with type 2 diabetes mellitus.Diabetol Metab Syndr. 2025 Jun 18;17(1):225. doi: 10.1186/s13098-025-01814-5. Diabetol Metab Syndr. 2025. PMID: 40533816 Free PMC article.
References
-
- Collaborators GBDRF Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659–1724. doi: 10.1016/S0140-6736(16)31679-8. - DOI - PMC - PubMed
-
- Tai ES, Ho SC, Fok AC, Tan CE. Measurement of obesity by anthropometry and bioelectric impedance analysis: correlation with fasting lipids and insulin resistance in an Asian population. Ann Acad Med Singap. 1999;28(3):445–450. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
