

Pelvic inlet area is associated with birth mode
- PMID: 36320156
- PMCID: PMC9780724
- DOI: 10.1111/aogs.14478
Pelvic inlet area is associated with birth mode
Abstract
Introduction: To determine whether a pelvis is wide enough for spontaneous delivery has long been the subject of obstetric research. A number of variables have been proposed as predictors, all with limited accuracy. In this study, we use a novel three-dimensional (3D) method to measure the female pelvis and assess which pelvic features influence birth mode. We compare the 3D pelvic morphology of women who delivered vaginally, women who had cesarean sections, and nulliparous women. The aim of this study is to identify differences in pelvic morphology between these groups.
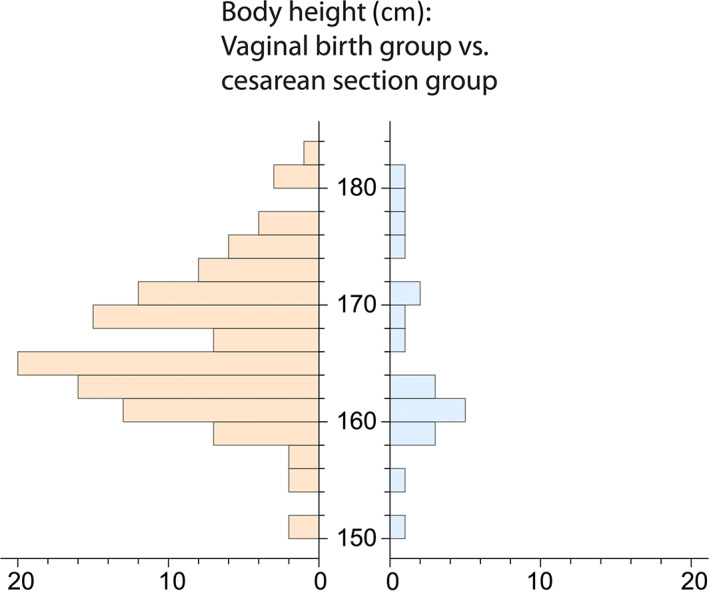
Material and methods: This observational study included women aged 50 years and older who underwent a CT scan of the pelvis for any medical indication. We recorded biometric data including height, weight, and age, and obtained the obstetric history. The bony pelvis was extracted from the CT scans and reconstructed in three dimensions. By placing 274 landmarks on each surface model, the pelvises were measured in detail. The pelvic inlet was measured using 32 landmarks. The trial was registered at the German Clinical Trials Register DRKS (DRKS00017690).
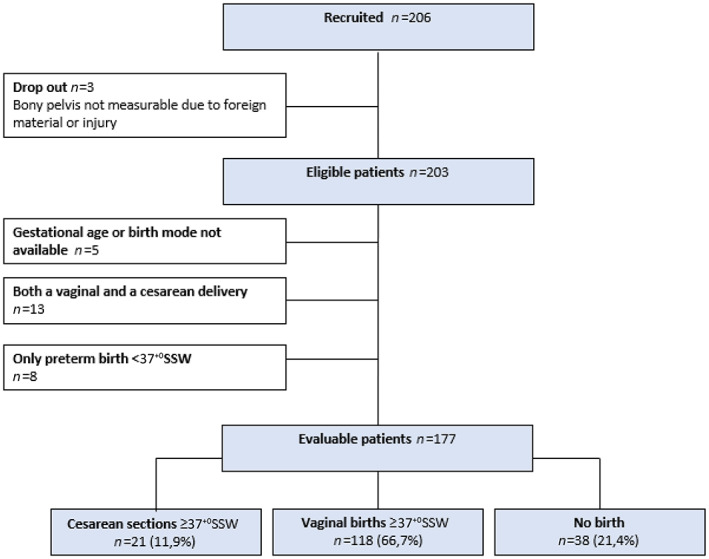
Results: For this study, 206 women were screened. Exclusion criteria were foreign material in the bony pelvis, unknown birth mode, and exclusively preterm births. Women who had both a vaginal birth and a cesarean section were excluded from the group comparison. We compared the pelvises of 177 women between three groups divided by obstetric history: vaginal births only (n = 118), cesarean sections only (n = 21), and nulliparous women (n = 38). The inlet area was significantly smaller in the cesarean section group (mean = 126.3 cm2 ) compared with the vaginal birth group (mean = 134.9 cm2 , p = 0.002). The nulliparous women were used as a control group: there was no statistically significant difference in pelvic inlet area between the nulliparous and vaginal birth groups.
Conclusions: By placing 274 landmarks on a pelvis reconstructed in 3D, a very precise measurement of the morphology of the pelvis is possible. We identified a significant difference in pelvic inlet area between women with vaginal delivery and those with cesarean section. A unique feature of this study is the method of measurement of the bony pelvis that goes beyond linear distance measurements as used in previous pelvimetric studies.
Keywords: birth mode; female pelvic morphology; fetopelvic disproportion; geometric morphometrics; pelvic inlet area; pelvimetry.
© 2022 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
TS reports a lecture fee by Ferring GmbH. SM reports research funding, advisory board, honorary or travel expenses: AbbVie, AstraZeneca, Clovis, Eisai, GlaxoSmithKline, Hubro, Medac, MSD, Novartis, Nykode, Olympus, PharmaMar, Pfizer, Roche, Sensor Kinesis, Teva, Tesaro. TK reports a relative employed at Roche, holds stock of Roche, Biontech, Valneva. The other authors declare that they have no competing interests.
Figures



Similar articles
-
MR pelvimetry: prognosis for successful vaginal delivery in patients with suspected fetopelvic disproportion or breech presentation at term.Arch Gynecol Obstet. 2017 Feb;295(2):351-359. doi: 10.1007/s00404-016-4276-6. Epub 2017 Jan 2. Arch Gynecol Obstet. 2017. PMID: 28044181
-
X-ray Pelvimetry Has No Impact on the Outcomes of Trial of Labor after Cesarean Delivery: A Retrospective Single-center Study.Kobe J Med Sci. 2024 Jun 19;70(2):E70-E76. doi: 10.24546/0100490211. Kobe J Med Sci. 2024. PMID: 38936881 Free PMC article.
-
MRI-based pelvimetric measurements as predictors for a successful vaginal breech delivery in the Frankfurt Breech at term cohort (FRABAT).Eur J Obstet Gynecol Reprod Biol. 2019 Jan;232:10-17. doi: 10.1016/j.ejogrb.2018.09.033. Epub 2018 Oct 22. Eur J Obstet Gynecol Reprod Biol. 2019. PMID: 30453166
-
Evolution of the human pelvis and obstructed labor: new explanations of an old obstetrical dilemma.Am J Obstet Gynecol. 2020 Jan;222(1):3-16. doi: 10.1016/j.ajog.2019.06.043. Epub 2019 Jun 25. Am J Obstet Gynecol. 2020. PMID: 31251927 Free PMC article. Review.
-
[Methods, techniques and assessment criteria in obstetric pelvimetry].Z Geburtshilfe Perinatol. 1994 Mar-Apr;198(2):37-46. Z Geburtshilfe Perinatol. 1994. PMID: 8023529 Review. German.
Cited by
-
There is an obstetrical dilemma: Misconceptions about the evolution of human childbirth and pelvic form.Am J Biol Anthropol. 2023 Aug;181(4):535-544. doi: 10.1002/ajpa.24802. Epub 2023 Jun 23. Am J Biol Anthropol. 2023. PMID: 37353889 Free PMC article. Review.
References
-
- Baird D. The cause and prevention of difficult labour. Am J Obstet Gynecol. 1952;63:1200‐1212. - PubMed
-
- Hofmeyr GJ. Obstructed labor: using better technologies to reduce mortality. Int J Gynaecol Obstet. 2004;85(Suppl 1):S62‐S72. - PubMed
-
- Burke N, Burke G, Breathnach F, et al. Prediction of cesarean delivery in the term nulliparous woman: results from the prospective, multicenter genesis study. Am J Obstet Gynecol. 2017;216:598.e1‐e11. - PubMed
-
- Bresler JB. Maternal height and the prevalence of stillbirths. Am J Phys Anthropol. 1962;20:515‐517. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
