

Speech and language characteristics differentiate Alzheimer's disease and dementia with Lewy bodies
- PMID: 36320609
- PMCID: PMC9614050
- DOI: 10.1002/dad2.12364
Speech and language characteristics differentiate Alzheimer's disease and dementia with Lewy bodies
Abstract
Introduction: Early differential diagnosis of Alzheimer's disease (AD) and dementia with Lewy bodies (DLB) is important, but it remains challenging. Different profiles of speech and language impairments between AD and DLB have been suggested, but direct comparisons have not been investigated.
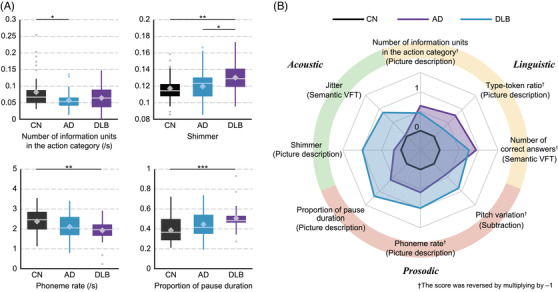
Methods: We collected speech responses from 121 older adults comprising AD, DLB, and cognitively normal (CN) groups and investigated their acoustic, prosodic, and linguistic features.
Results: The AD group showed larger differences from the CN group than the DLB group in linguistic features, while the DLB group showed larger differences in prosodic and acoustic features. Machine-learning classifiers using these speech features achieved 87.0% accuracy for AD versus CN, 93.2% for DLB versus CN, and 87.4% for AD versus DLB.
Discussion: Our findings indicate the discriminative differences in speech features in AD and DLB and the feasibility of using these features in combination as a screening tool for identifying/differentiating AD and DLB.
Keywords: acoustic; digital health; language impairment; linguistic; machine learning; natural language processing; prosodic; spontaneous speech.
© 2022 The Authors. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring published by Wiley Periodicals, LLC on behalf of Alzheimer's Association.
Conflict of interest statement
YY is employed by the IBM Corporation.KS is employed by the IBM Corporation.MN received funding from the Japan Society for the Promotion of Science, KAKENHI (grant number 19H01084).MO has nothing to disclose.KN has nothing to disclose.TA received funding from Japan Society for the Promotion of Science, KAKENHI (grant number 19H01084). TA reports honoraria for lectures from Eisai, Daiichi‐Sankyo, and Sumitomo Pharma. Author disclosures are available in the Supporting Information.
Figures
References
-
- McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):263‐269. 10.1016/j.jalz.2011.03.005 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources