

Impact of belatacept and tacrolimus on cytomegalovirus viral load control and relapse in moderate and high-risk cytomegalovirus serostatus kidney transplant recipients
- PMID: 36321801
- PMCID: PMC10078597
- DOI: 10.1111/tid.13983
Impact of belatacept and tacrolimus on cytomegalovirus viral load control and relapse in moderate and high-risk cytomegalovirus serostatus kidney transplant recipients
Abstract
Background: Belatacept improves long-term graft survival, but control of some primary viral infections may be impaired. We evaluated the impact of belatacept and tacrolimus on cytomegalovirus (CMV) viral control, remission and relapse in CMV high-risk and moderate-risk recipients.
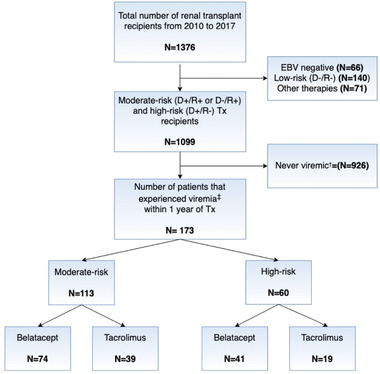
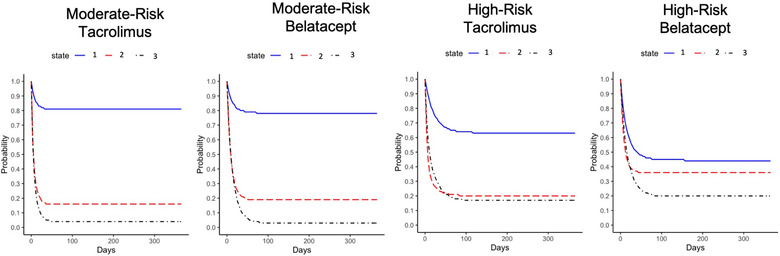
Methods: Using a multistate Markov model, we evaluated viral load state transitions of 173 kidney transplant recipients with at least one episode of viremia within 1 year after transplant: state 1, undetectable/low viral load; state 2, moderate viremia; and state 3, severe viremia.
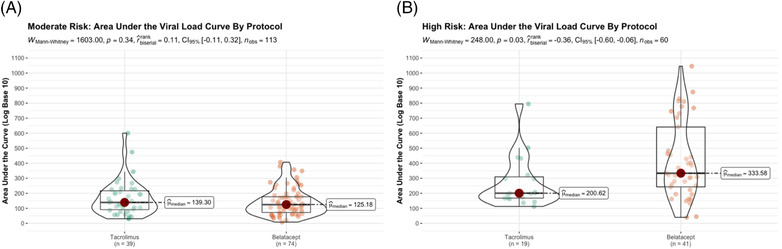
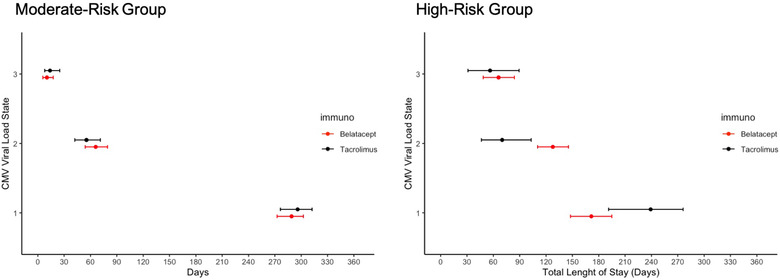
Results: Among high-risk recipients, belatacept-treated recipients exhibited a significantly higher probability of entering moderate viremia (.36; 95% CI = .31, .41) than tacrolimus-treated recipients (.20; 95% CI = .13, .29). The expected number of days in viremic states differed. High-risk belatacept-treated recipients persisted in moderate viremia for significantly longer (128 days, 95% CI = 110, 146) than did tacrolimus-treated recipients (70.0 days, 95% CI = 45.2, 100) and showed a trend of shorter duration in low/undetectable viral load state (172 days, 95% CI = 148, 195) than did tacrolimus-treated recipients (239 days, 95% CI = 195, 277). Moderate-risk recipients showed better viral load control and with no differences by immunosuppression.
Conclusion: High-risk belatacept-treated recipients showed defects in sustaining viral control relative to tacrolimus-treated recipients. Avoidance of initial use belatacept in high-risk recipients or development of modified management protocols should be considered.
Keywords: CMV bidirectional viral load state transitions; CMV control; CMV high-risk; CMV management strategies; CMV moderate-risk; CMV relapse; CMV serostatus risk; CMV viral infection and infectious agents; CMV viral load dynamics; CMV viral load volatility; Markov multistate; belatacept; clinical research/practice; cytomegalovirus; immunosuppression/immune modulation; immunosuppressive regimens-maintenance; infectious disease; kidney (allograft) function/disfunction; kidney transplant; length of stay in viral load state; tacrolimus; viral load trajectory; viremia.
© 2022 The Authors. Transplant Infectious Disease published by Wiley Periodicals LLC.
Conflict of interest statement
All authors in this manuscript declared no conflict of interest.
Figures
References
-
- Heldenbrand S, Li C, Cross RP, et al. Multicenter evaluation of efficacy and safety of low‐dose versus high‐dose valganciclovir for prevention of cytomegalovirus disease in donor and recipient positive (D+/R+) renal transplant recipients. Transpl Infect Dis. 2016;18(6):904‐912. 10.1111/tid.12609 - DOI - PubMed
