

Conditioning Regimens are Associated with Distinct Patterns of Microbiota Injury in Allogeneic Hematopoietic Cell Transplantation
- PMID: 36322005
- PMCID: PMC9812902
- DOI: 10.1158/1078-0432.CCR-22-1254
Conditioning Regimens are Associated with Distinct Patterns of Microbiota Injury in Allogeneic Hematopoietic Cell Transplantation
Abstract
Purpose: The gut microbiota is subject to multiple insults in allogeneic hematopoietic cell transplantation (allo-HCT) recipients. We hypothesized that preparative conditioning regimens contribute to microbiota perturbation in allo-HCT.
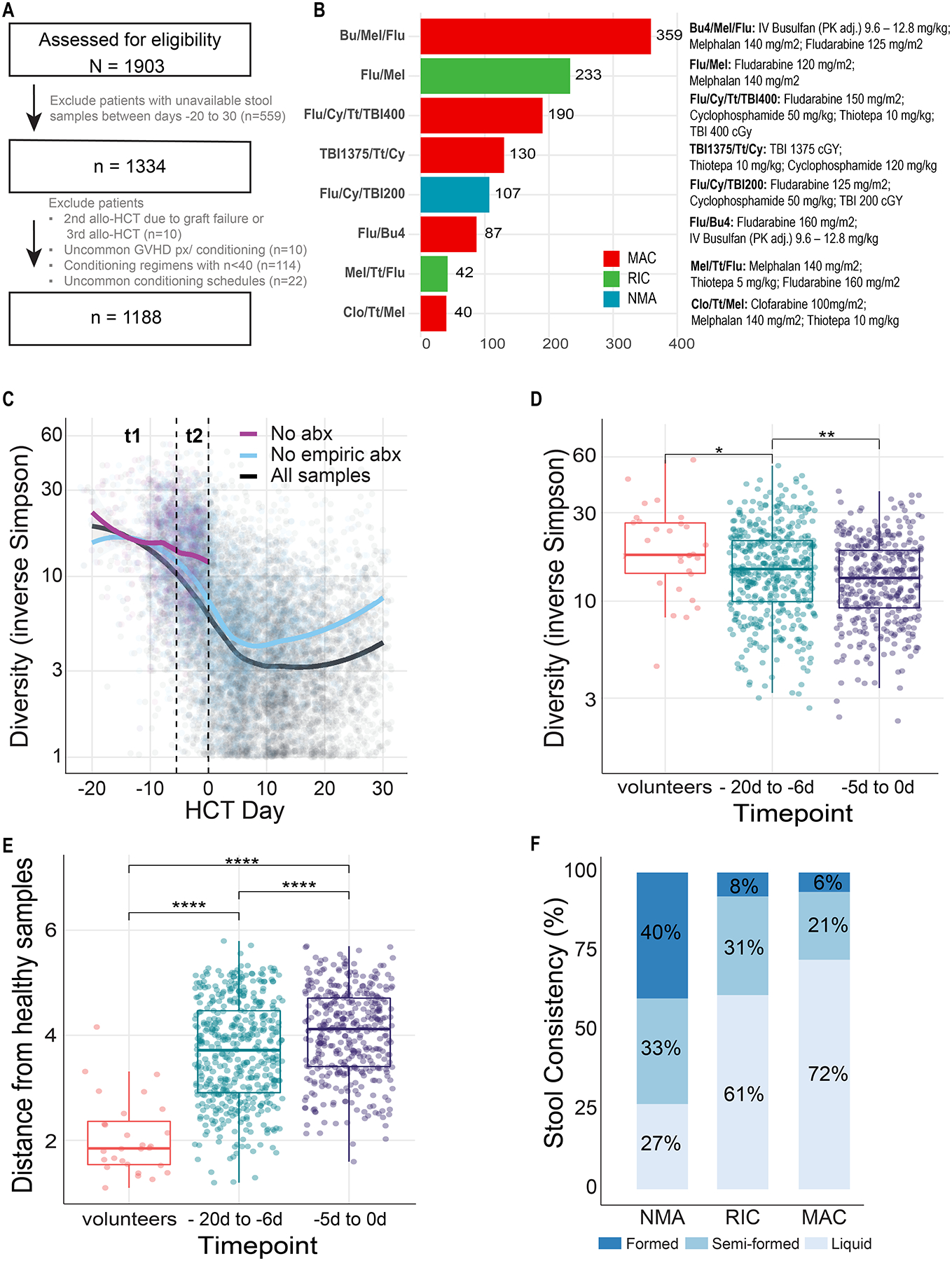
Experimental design: This was a retrospective study that evaluated the relationship between conditioning regimens exposure in 1,188 allo-HCT recipients and the gut microbiome. Stool samples collected from 20 days before transplantation up to 30 days after were profiled using 16S rRNA sequencing. Microbiota injury was quantified by changes in α-diversity.
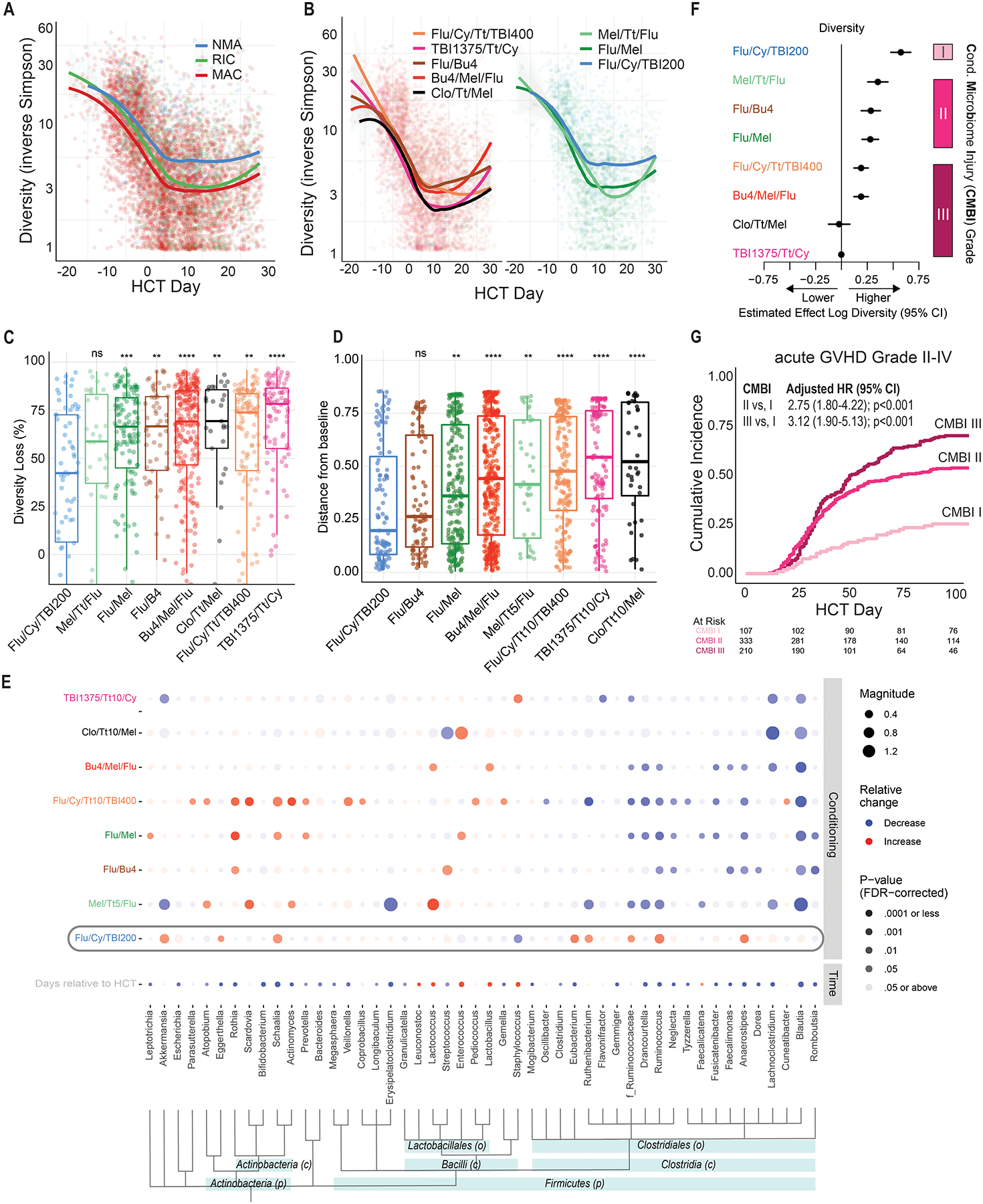
Results: We identified distinct patterns of microbiota injury that varied by conditioning regimen. Diversity loss was graded into three levels of conditioning-associated microbiota injury (CMBI) in a multivariable model that included antibiotic exposures. High-intensity regimens, such as total body irradiation (TBI)-thiotepa-cyclophosphamide, were associated with the greatest injury (CMBI III). In contrast, the nonmyeloablative regimen fludarabine-cyclophosphamide with low-dose TBI (Flu/Cy/TBI200) had a low-grade injury (CMBI I). The risk of acute GVHD correlated with CMBI degree. Pretransplant microbial compositions were best preserved with Flu/Cy/TBI200, whereas other regimens were associated with loss of commensal bacteria and expansion of Enterococcus.
Conclusions: Our findings support an interaction between conditioning at the regimen level and the extent of microbiota injury.
©2022 American Association for Cancer Research.
Figures
References
-
- Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, et al. Defining the intensity of conditioning regimens: working definitions. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation 2009;15(12):1628–33 doi 10.1016/j.bbmt.2009.07.004. - DOI - PMC - PubMed
-
- Giralt S, Ballen K, Rizzo D, Bacigalupo A, Horowitz M, Pasquini M, et al. Reduced-intensity conditioning regimen workshop: defining the dose spectrum. Report of a workshop convened by the center for international blood and marrow transplant research. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation 2009;15(3):367–9 doi 10.1016/j.bbmt.2008.12.497. - DOI - PMC - PubMed
-
- Cooke KR, Luznik L, Sarantopoulos S, Hakim FT, Jagasia M, Fowler DH, et al. The biology of chronic graft-versus-host disease: a task force report from the National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease. Biology of Blood and Marrow Transplantation 2017;23(2):211–34. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
