

Once-Weekly Semaglutide in Adolescents with Obesity
- PMID: 36322838
- PMCID: PMC9997064
- DOI: 10.1056/NEJMoa2208601
Once-Weekly Semaglutide in Adolescents with Obesity
Abstract
Background: A once-weekly, 2.4-mg dose of subcutaneous semaglutide, a glucagon-like peptide-1 receptor agonist, is used to treat obesity in adults, but assessment of the drug in adolescents has been lacking.
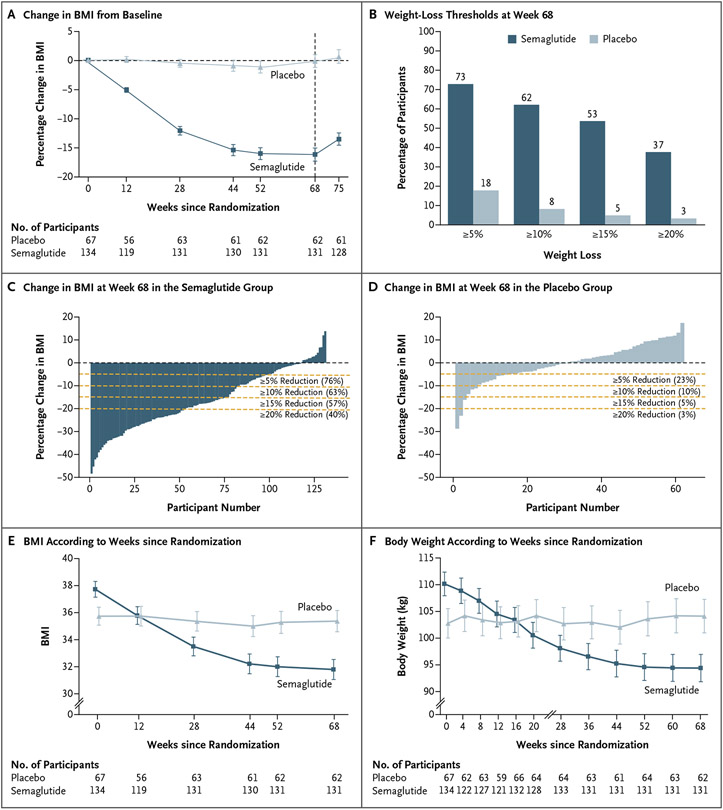
Methods: In this double-blind, parallel-group, randomized, placebo-controlled trial, we enrolled adolescents (12 to <18 years of age) with obesity (a body-mass index [BMI] in the 95th percentile or higher) or with overweight (a BMI in the 85th percentile or higher) and at least one weight-related coexisting condition. Participants were randomly assigned in a 2:1 ratio to receive once-weekly subcutaneous semaglutide (at a dose of 2.4 mg) or placebo for 68 weeks, plus lifestyle intervention. The primary end point was the percentage change in BMI from baseline to week 68; the secondary confirmatory end point was weight loss of at least 5% at week 68.
Results: A total of 201 participants underwent randomization, and 180 (90%) completed treatment. All but one of the participants had obesity. The mean change in BMI from baseline to week 68 was -16.1% with semaglutide and 0.6% with placebo (estimated difference, -16.7 percentage points; 95% confidence interval [CI], -20.3 to -13.2; P<0.001). At week 68, a total of 95 of 131 participants (73%) in the semaglutide group had weight loss of 5% or more, as compared with 11 of 62 participants (18%) in the placebo group (estimated odds ratio, 14.0; 95% CI, 6.3 to 31.0; P<0.001). Reductions in body weight and improvement with respect to cardiometabolic risk factors (waist circumference and levels of glycated hemoglobin, lipids [except high-density lipoprotein cholesterol], and alanine aminotransferase) were greater with semaglutide than with placebo. The incidence of gastrointestinal adverse events was greater with semaglutide than with placebo (62% vs. 42%). Five participants (4%) in the semaglutide group and no participants in the placebo group had cholelithiasis. Serious adverse events were reported in 15 of 133 participants (11%) in the semaglutide group and in 6 of 67 participants (9%) in the placebo group.
Conclusions: Among adolescents with obesity, once-weekly treatment with a 2.4-mg dose of semaglutide plus lifestyle intervention resulted in a greater reduction in BMI than lifestyle intervention alone. (Funded by Novo Nordisk; STEP TEENS ClinicalTrials.gov number, NCT04102189.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
Once-Weekly Semaglutide in Adolescents with Obesity.N Engl J Med. 2023 Mar 23;388(12):1145. doi: 10.1056/NEJMc2300510. N Engl J Med. 2023. PMID: 36947474 No abstract available.
-
Once-Weekly Semaglutide in Adolescents with Obesity.N Engl J Med. 2023 Mar 23;388(12):1145-1146. doi: 10.1056/NEJMc2300510. N Engl J Med. 2023. PMID: 36947475 No abstract available.
-
Once-Weekly Semaglutide in Adolescents with Obesity. Reply.N Engl J Med. 2023 Mar 23;388(12):1146. doi: 10.1056/NEJMc2300510. N Engl J Med. 2023. PMID: 36947476 No abstract available.
References
-
- Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process: a position statement of the World Obesity Federation. Obes Rev 2017; 18:715–23. - PubMed
-
- Daniels SR, Arnett DK, Eckel RH, et al. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation 2005;111: 1999–2012. - PubMed
-
- Small L, Aplasca A. Child obesity and mental health: a complex interaction. Child Adolesc Psychiatr Clin N Am 2016; 25:269–82. - PubMed
-
- World Obesity Federation. World obesity atlas 2022. March 2022. (https://www.worldobesity.org/resources/resource-library/world-obesity-at...).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical