

Germ line DDX41 mutations define a unique subtype of myeloid neoplasms
- PMID: 36322930
- PMCID: PMC10935555
- DOI: 10.1182/blood.2022018221
Germ line DDX41 mutations define a unique subtype of myeloid neoplasms
Erratum in
-
Makishima H, Saiki R, Nannya Y, et al. Germ line DDX41 mutations define a unique subtype of myeloid neoplasms. Blood. 2023;141(5):534-549.Blood. 2024 May 2;143(18):1879. doi: 10.1182/blood.2024024462. Blood. 2024. PMID: 38696198 Free PMC article. No abstract available.
Abstract
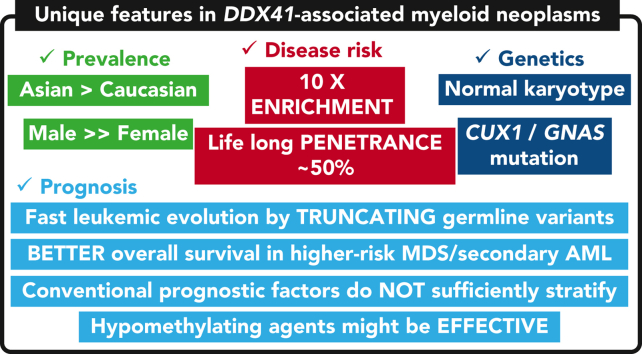
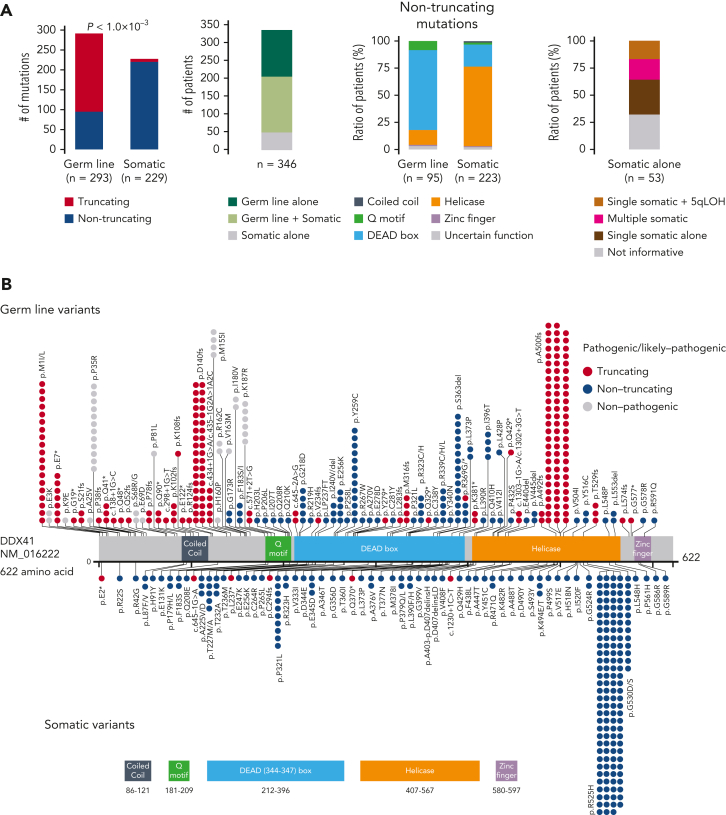
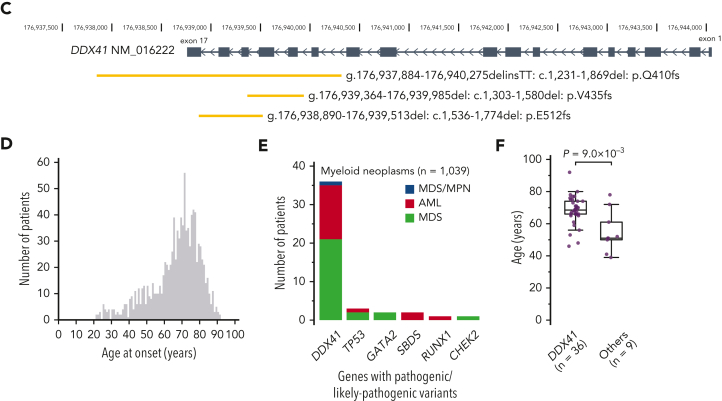
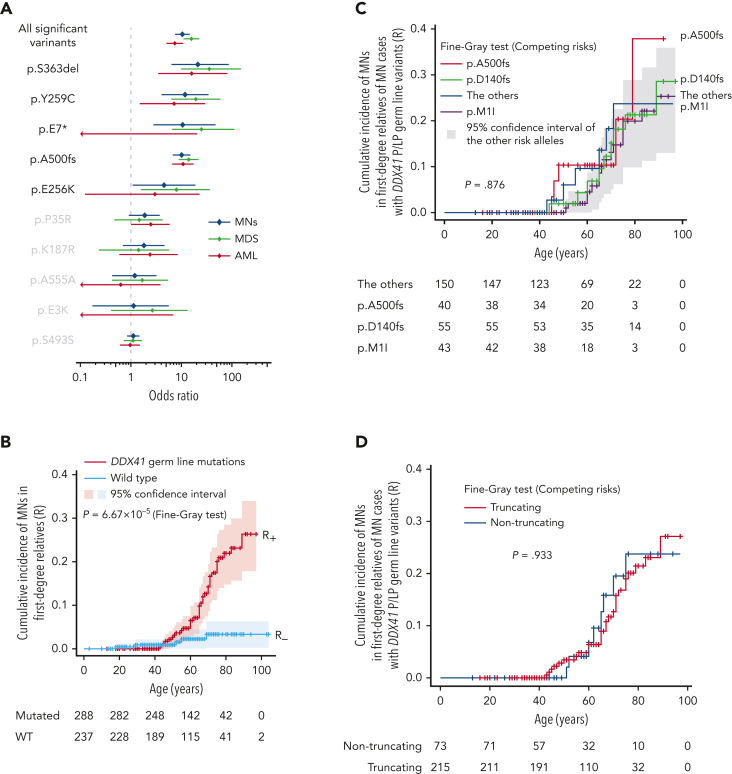
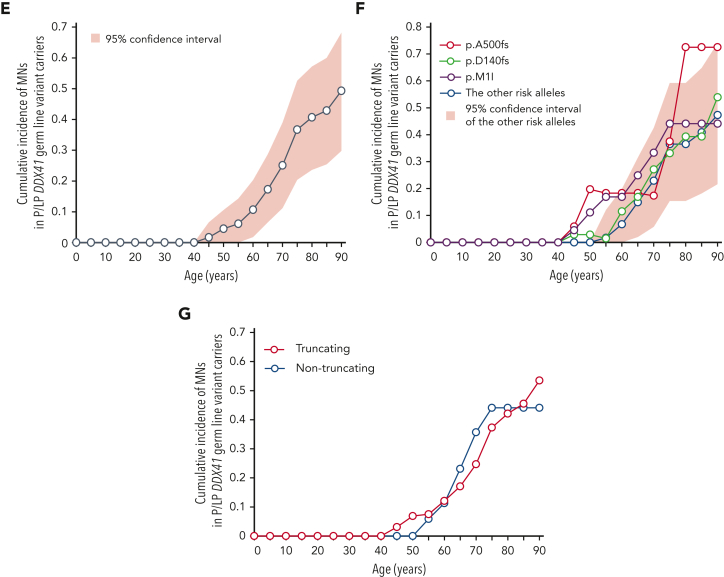
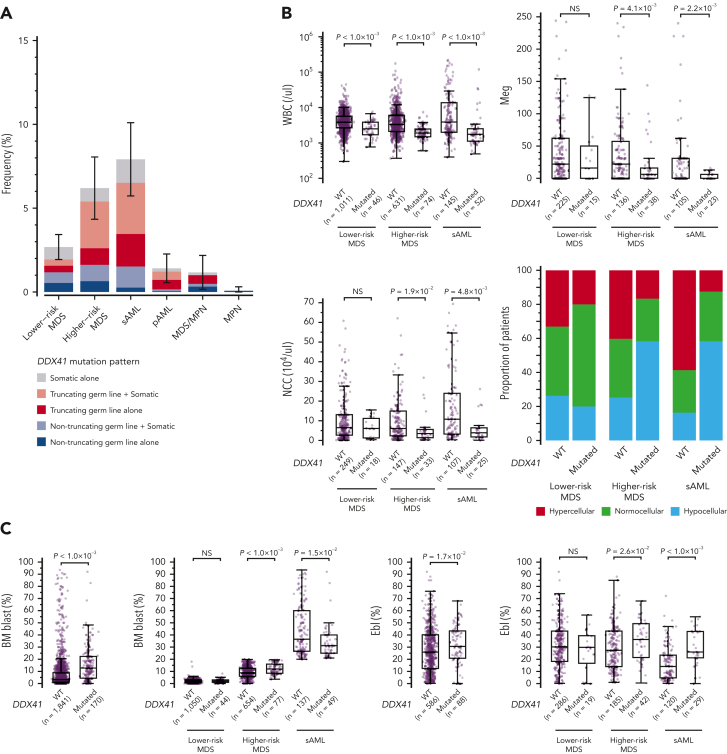
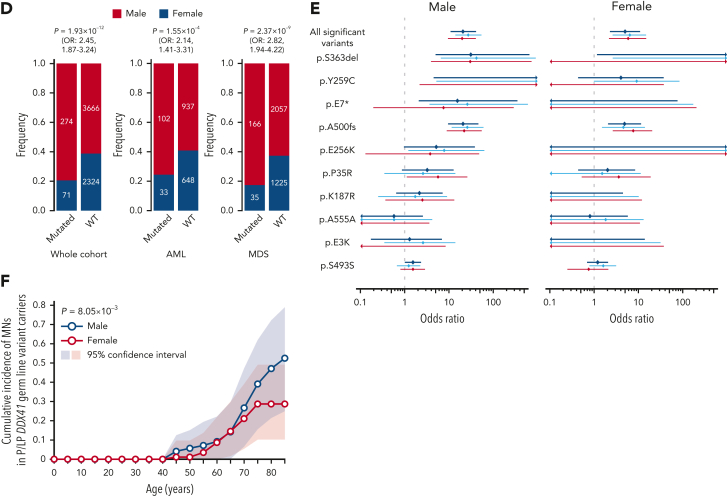
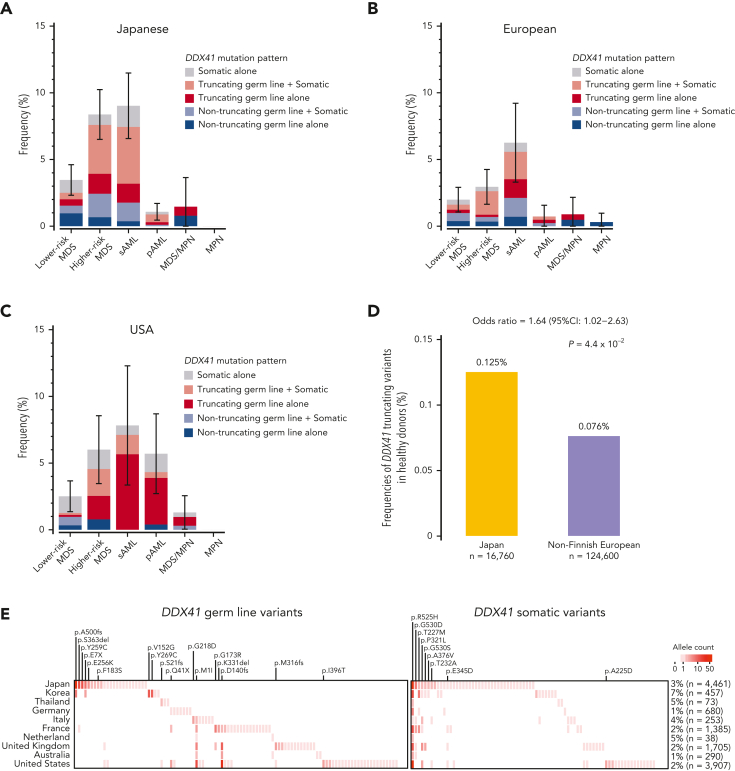
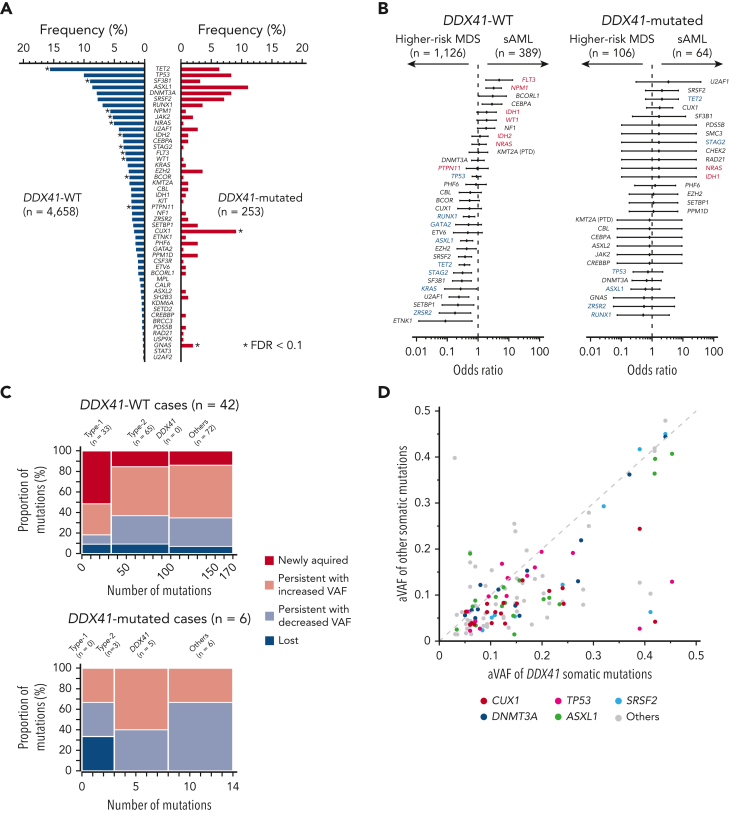
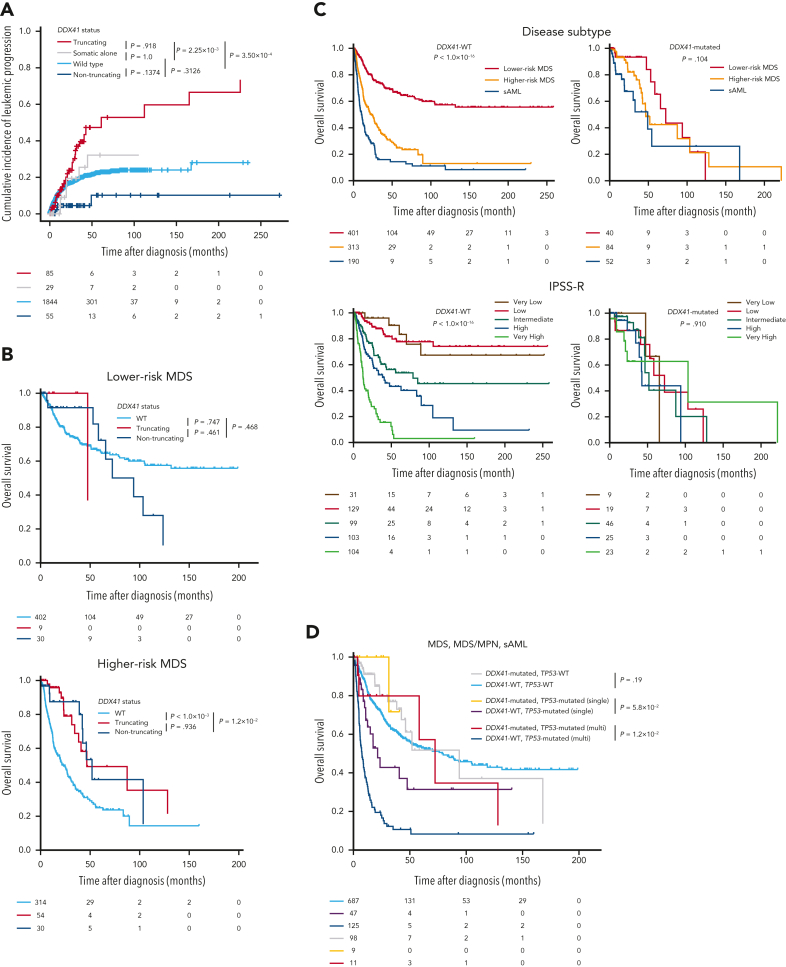
Germ line DDX41 variants have been implicated in late-onset myeloid neoplasms (MNs). Despite an increasing number of publications, many important features of DDX41-mutated MNs remain to be elucidated. Here we performed a comprehensive characterization of DDX41-mutated MNs, enrolling a total of 346 patients with DDX41 pathogenic/likely-pathogenic (P/LP) germ line variants and/or somatic mutations from 9082 MN patients, together with 525 first-degree relatives of DDX41-mutated and wild-type (WT) patients. P/LP DDX41 germ line variants explained ∼80% of known germ line predisposition to MNs in adults. These risk variants were 10-fold more enriched in Japanese MN cases (n = 4461) compared with the general population of Japan (n = 20 238). This enrichment of DDX41 risk alleles was much more prominent in male than female (20.7 vs 5.0). P/LP DDX41 variants conferred a large risk of developing MNs, which was negligible until 40 years of age but rapidly increased to 49% by 90 years of age. Patients with myelodysplastic syndromes (MDS) along with a DDX41-mutation rapidly progressed to acute myeloid leukemia (AML), which was however, confined to those having truncating variants. Comutation patterns at diagnosis and at progression to AML were substantially different between DDX41-mutated and WT cases, in which none of the comutations affected clinical outcomes. Even TP53 mutations made no exceptions and their dismal effect, including multihit allelic status, on survival was almost completely mitigated by the presence of DDX41 mutations. Finally, outcomes were not affected by the conventional risk stratifications including the revised/molecular International Prognostic Scoring System. Our findings establish that MDS with DDX41-mutation defines a unique subtype of MNs that is distinct from other MNs.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.O.: Leadership position/advisory role for: KAN Research Institute, Inc, ChordiaTherapeutics, Inc. Stockholder in: Asahi Genomics Co, Ltd. Grant/Research funding from: KAN Research Institute, Inc, ChordiaTherapeutics, Inc, Sumitomo Dainippon Pharma Co, Ltd, Otsuka Pharmaceutical Co, Ltd, Eisai Co, Ltd. Accepted a researcher from: ChordiaTherapeutics, Inc. The remaining authors declare no competing financial interests.
Figures
Comment in
-
DDX41: the poster child for familial MDS/AML grows up.Blood. 2023 Feb 2;141(5):447-449. doi: 10.1182/blood.2022018787. Blood. 2023. PMID: 36729548 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
