

Lumbar cistern Candida intradural abscess following epidural anesthesia
- PMID: 36324960
- PMCID: PMC9610685
- DOI: 10.25259/SNI_750_2022
Lumbar cistern Candida intradural abscess following epidural anesthesia
Abstract
Background: This report describes a case of an immunocompetent patient with an intradural abscess from Candida dubliniensis. The majority of fungal spine infections, although rare in general, are due to Aspergillus or C. albicans through systemic fungemia. To date, there have only been two reports of spondylodiscitis from C. dubliniensis.
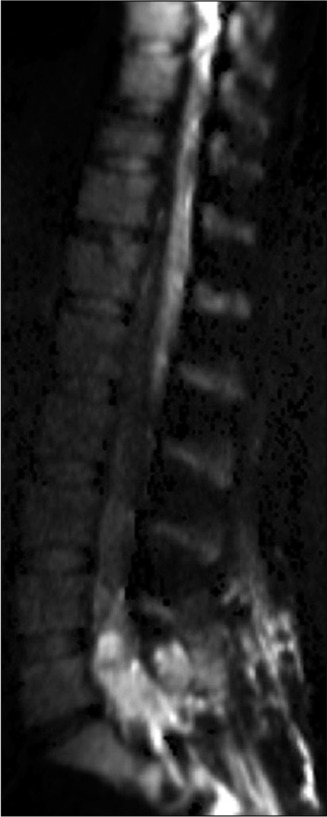
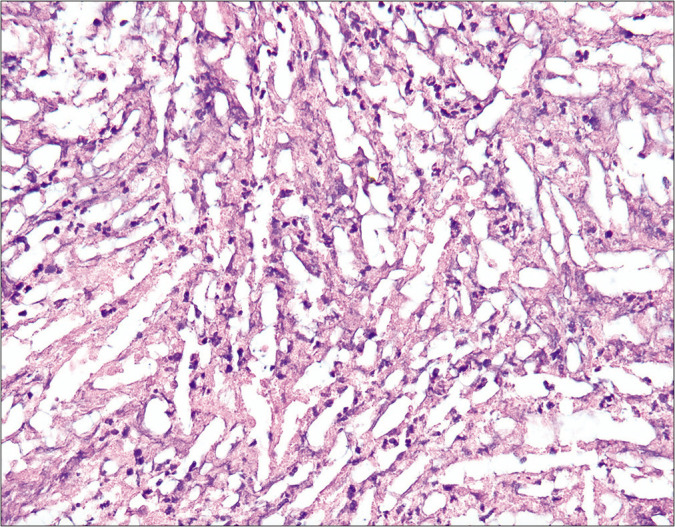
Case description: A 37-year-old immunocompetent female patient presented to the neurosurgical service for worsening headaches with nausea, vomiting, vision changes, and weight loss. MRI studies showed diffuse leptomeningeal enhancement of the distal spinal cord, conus medullaris, and nerve roots of the cauda equina extending beyond the neural foramina bilaterally. She had persistent symptoms and no clear diagnosis on lumbar puncture or systemic testing therefore L5-S1 laminectomy for an intradural tissue biopsy was performed. During surgery, cultures were taken and grew colonies of C. dubliniensis.
Conclusion: This organism has been reported rarely in the literature as being an infectious agent, thus diagnosing remains a challenge but should be considered in patients with a suggestive history.
Keywords: Candida dubliniensis; Cauda equina; Intradural abscess; Spinal abscess.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
Presentation of cauda equina syndrome due to an intradural extramedullary abscess: a case report.Spine J. 2014 Feb 1;14(2):e1-6. doi: 10.1016/j.spinee.2013.09.029. Epub 2013 Oct 17. Spine J. 2014. PMID: 24331844 Review.
-
Intradural cauda equina Candida abscess presenting with hydrocephalus: case report.J Neurosurg Spine. 2019 Aug 30;31(6):890-893. doi: 10.3171/2019.6.SPINE19271. Print 2019 Dec 1. J Neurosurg Spine. 2019. PMID: 31470401 Free PMC article.
-
Case Report: Candida dubliniensis as a Cause of Chronic Meningitis.Front Neurol. 2020 Dec 8;11:601242. doi: 10.3389/fneur.2020.601242. eCollection 2020. Front Neurol. 2020. PMID: 33363510 Free PMC article.
-
A rare case of intradural and extramedullary epidermoid cyst after repetitive epidural anesthesia: case report and review of the literature.World J Surg Oncol. 2017 Jul 17;15(1):131. doi: 10.1186/s12957-017-1186-4. World J Surg Oncol. 2017. PMID: 28716031 Free PMC article. Review.
-
Intradural Candida Albicans infection that presented as epidural abscess: A case report.Int J Surg Case Rep. 2023 Jun;107:108337. doi: 10.1016/j.ijscr.2023.108337. Epub 2023 May 18. Int J Surg Case Rep. 2023. PMID: 37210802 Free PMC article.
References
-
- Chia SL, Tan BH, Tan CT, Tan SB. Candida spondylodiscitis and epidural abscess: Management with shorter courses of anti-fungal therapy in combination with surgical debridement. J Infect. 2005;51:17–23. - PubMed
-
- Kauffman CA, Malani AN. Fungal infections associated with contaminated steroid injections. Microbiol Spectr. 2016;4:1–13. - PubMed
-
- Kulkarni AG, Chu G, Fehlings MG. Pyogenic intradural abcess: A case report. Spine (Phila Pa 1976) 2008;32:E354–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources