

TCR repertoire profiling revealed antigen-driven CD8+ T cell clonal groups shared in synovial fluid of patients with spondyloarthritis
- PMID: 36325356
- PMCID: PMC9618624
- DOI: 10.3389/fimmu.2022.973243
TCR repertoire profiling revealed antigen-driven CD8+ T cell clonal groups shared in synovial fluid of patients with spondyloarthritis
Abstract
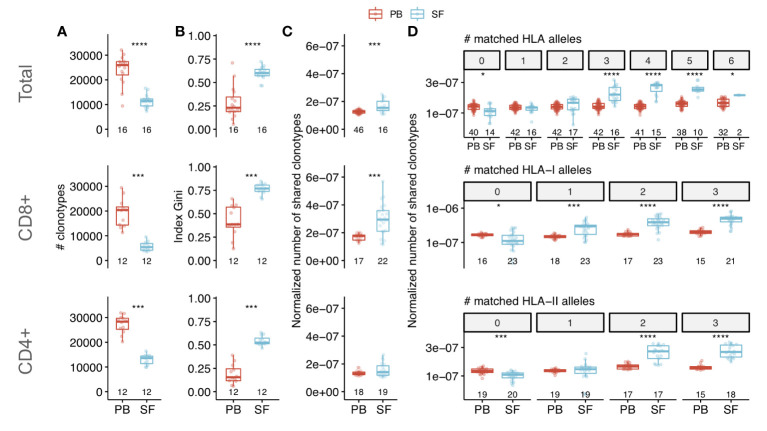
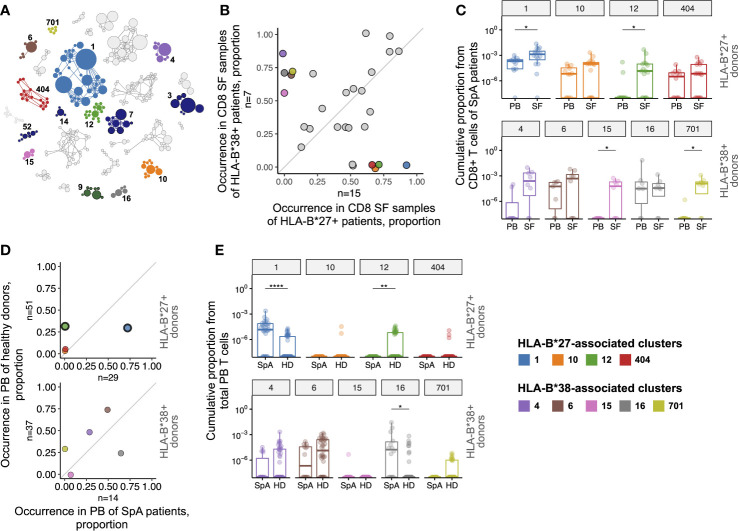
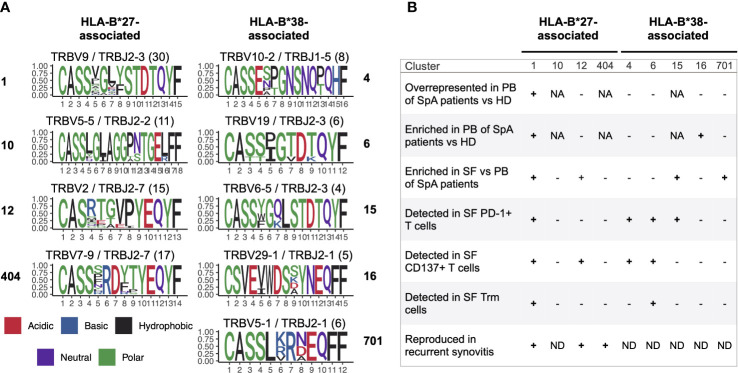
Spondyloarthritis (SpA) comprises a number of inflammatory rheumatic diseases with overlapping clinical manifestations. Strong association with several HLA-I alleles and T cell infiltration into an inflamed joint suggest involvement of T cells in SpA pathogenesis. In this study, we performed high-throughput T cell repertoire profiling of synovial fluid (SF) and peripheral blood (PB) samples collected from a large cohort of SpA patients. We showed that synovial fluid is enriched with expanded T cell clones that are shared between patients with similar HLA genotypes and persist during recurrent synovitis. Using an algorithm for identification of TCRs involved in immune response we discovered several antigen-driven CD8+ clonal groups associated with risk HLA-B*27 or HLA-B*38 alleles. We further show that these clonal groups were enriched in SF and had higher frequency in PB of SpA patients vs healthy donors, implying their relevance to SpA pathogenesis. Several of the groups were shared among patients with different SpAs that suggests a common immunopathological mechanism of the diseases. In summary, our results provide evidence for the role of specific CD8+ T cell clones in pathogenesis of SpA.
Keywords: TCR repertoire; ankylosing spondylitis; psoriatic arthritis; spondyloarthritis; synovial fluid.
Copyright © 2022 Komech, Koltakova, Barinova, Minervina, Salnikova, Shmidt, Korotaeva, Loginova, Erdes, Bogdanova, Shugay, Lukyanov, Lebedev and Zvyagin.
Conflict of interest statement
EL is a member of the Speakers bureau of Janssen. TK is a member of Speakers bureau of: Pfizer, MSD, Novartis, AbbVie, Janssen, Lilly, Celgene, JSC BIOCAD, and Novartis-Sandoz. SE is a member of the Speaker’s bureau of KRKKA, MCB and JSC BIOCAD. SL and IZ provide scientific advice for JSC BIOCAD. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Landewé R, Sieper J, Mease P, Inman RD, Lambert RG, Deodhar A, et al. . Efficacy and safety of continuing versus withdrawing adalimumab therapy in maintaining remission in patients with non-radiographic axial spondyloarthritis (ABILITY-3): a multicentre, randomised, double-blind study. Lancet (2018) 392(10142):134–44. doi: 10.1016/S0140-6736(18)31362-X - DOI - PubMed
-
- Landewé RB, Gensler LS, Poddubnyy D, Rahman P, Hojnik M, Li X, et al. . Continuing versus withdrawing ixekizumab treatment in patients with axial spondyloarthritis who achieved remission: efficacy and safety results from a placebo-controlled, randomised withdrawal study (COAST-y). Ann Rheum Dis (2021) 80(8):1022–30. doi: 10.1136/annrheumdis-2020-219717 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials