

Weight change and clinical outcomes in heart failure with reduced ejection fraction: insights from EMPEROR-Reduced
- PMID: 36325584
- PMCID: PMC10098519
- DOI: 10.1002/ejhf.2728
Weight change and clinical outcomes in heart failure with reduced ejection fraction: insights from EMPEROR-Reduced
Erratum in
-
Corrigendum to 'Weight change and clinical outcomes in heart failure with reduced ejection fraction: Insights from EMPEROR-Reduced' [Eur J Heart Fail 2023;25:117-127].Eur J Heart Fail. 2023 Jun;25(6):924. doi: 10.1002/ejhf.2910. Epub 2023 Jun 5. Eur J Heart Fail. 2023. PMID: 37278104 Free PMC article. No abstract available.
Abstract
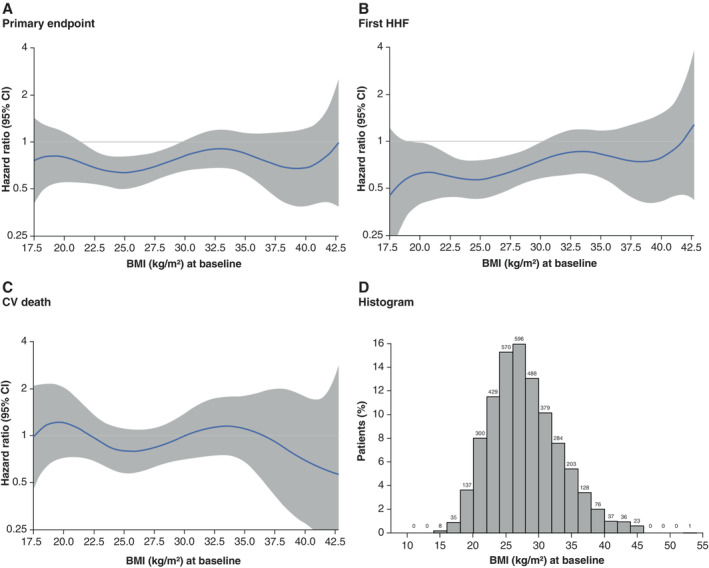
Aims: Baseline body mass index (BMI) and weight loss promoted by sodium-glucose cotransporter 2 inhibitors may impact outcomes in patients with heart failure with reduced ejection fraction (HFrEF). We assessed in the EMPEROR-Reduced population treated with empagliflozin versus placebo the relationship between baseline BMI, weight loss and effects on the primary (time to first hospitalization for heart failure [HHF] or cardiovascular death) and key secondary outcomes.
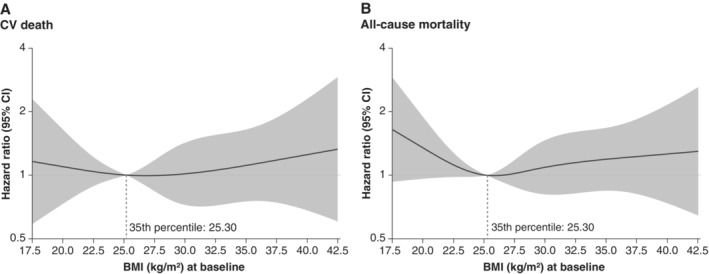
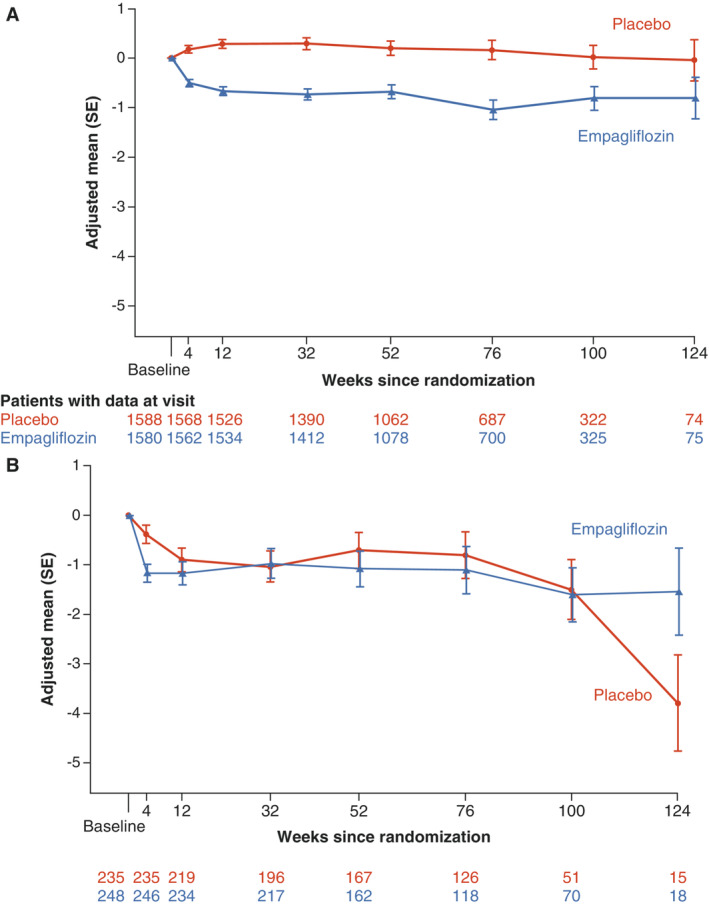
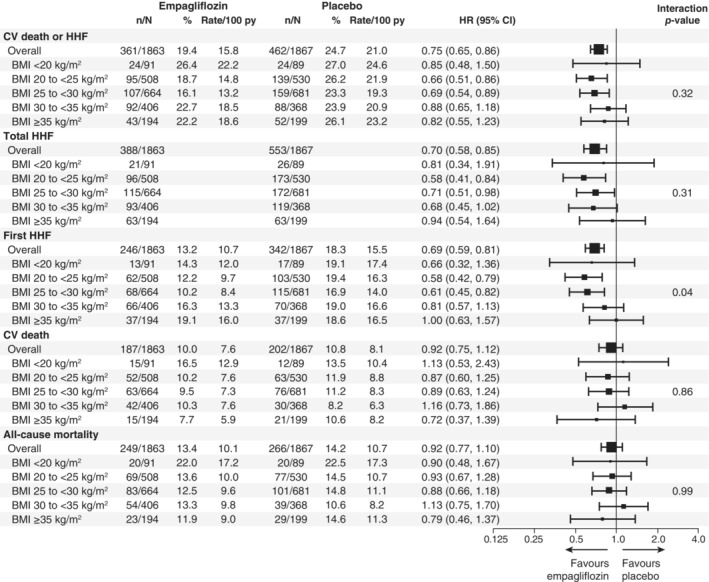
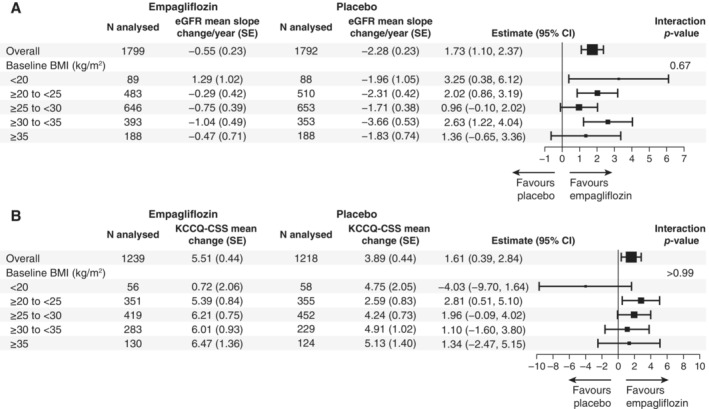
Methods and results: We categorized patients according to their baseline BMI: <20 kg/m2 (n = 180); 20 to <25 kg/m2 (n = 1038); 25 to <30 kg/m2 (n = 1345); 30 to <35 kg/m2 (n = 774) and ≥35 kg/m2 (n = 393). The treatment effect of empagliflozin on the primary outcome was consistent across all BMI categories (hazard ratios in subgroups 0.66-0.88, interaction trend p = 0.32), as was the effect on total (first plus recurrent) HHF (interaction trend p = 0.31). Empagliflozin reduced the rate of estimated glomerular filtration rate decline consistently across the BMI categories (interaction trend p = 0.67). Overall, incidence rates of any or serious adverse events were comparable between the treatment groups across all BMI categories. A total of 313 (17.4%) patients treated with empagliflozin experienced a weight loss of more than 5% at week 52 versus 230 (12.8%) in placebo. When analysed separately within each treatment group, presence of weight loss was similarly associated with an increased risk of all-cause mortality.
Conclusion: The benefits of empagliflozin versus placebo were consistently present across all BMI categories in HFrEF patients. Weight loss was associated with higher risk of all-cause mortality, regardless of treatment group.
Keywords: Body mass index; Empagliflozin; Heart failure; Weight loss.
© 2022 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Comment in
-
Weighing in on weight loss in heart failure with reduced ejection fraction.Eur J Heart Fail. 2023 Jan;25(1):128-130. doi: 10.1002/ejhf.2753. Epub 2023 Jan 4. Eur J Heart Fail. 2023. PMID: 36519663 Free PMC article. No abstract available.
References
-
- Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305–13. - PubMed
-
- Powell‐Wiley TM, Poirier P, Burke LE, Despres JP, Gordon‐Larsen P, Lavie CJ, et al.; American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; and Stroke Council . Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984–e1010. - PMC - PubMed
-
- Wong C, Marwick TH. Obesity cardiomyopathy: pathogenesis and pathophysiology. Nat Clin Pract Cardiovasc Med. 2007;4:436–43. - PubMed
