

Persistent High Burden of Heart Failure Across the Ejection Fraction Spectrum in a Nationwide Setting
- PMID: 36326055
- PMCID: PMC9750084
- DOI: 10.1161/JAHA.122.026708
Persistent High Burden of Heart Failure Across the Ejection Fraction Spectrum in a Nationwide Setting
Abstract
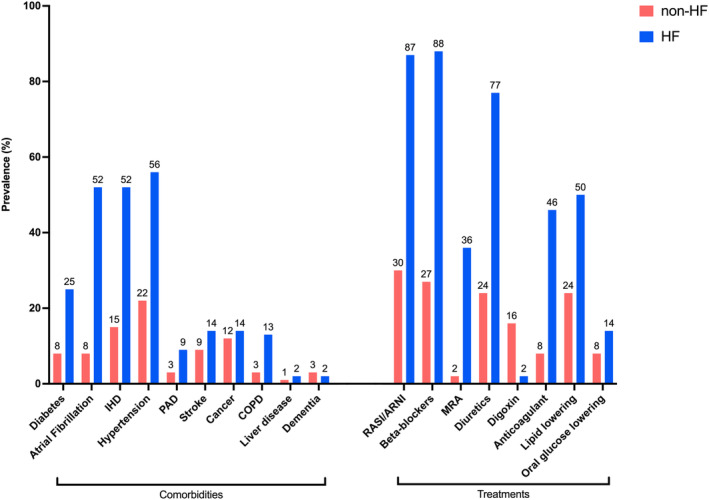
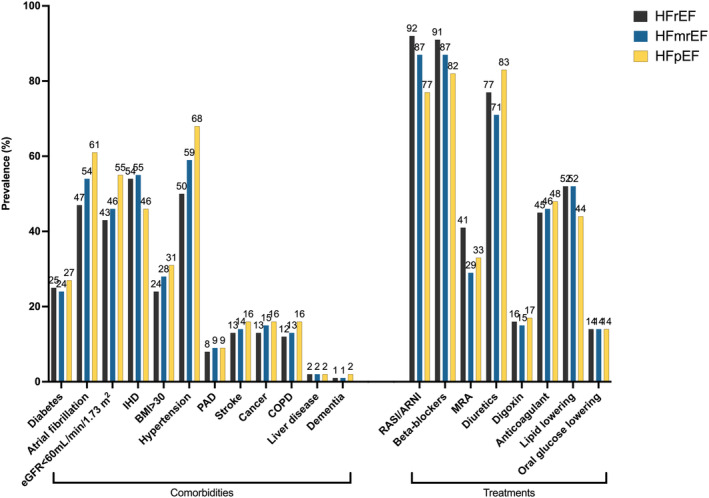
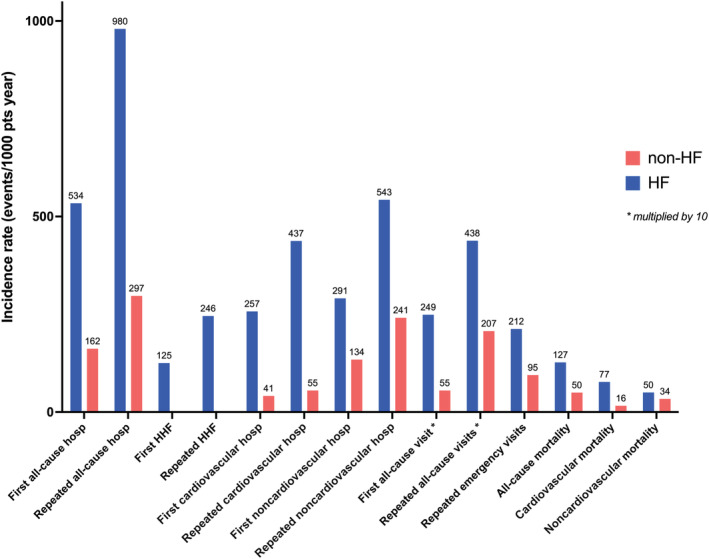
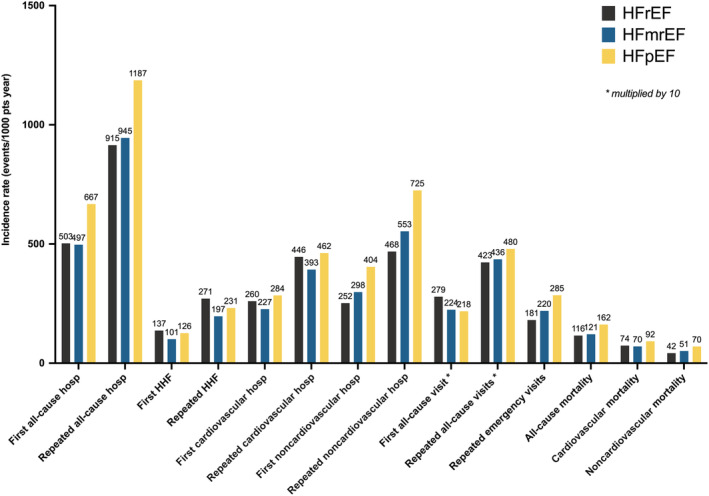
Background Heart failure (HF) has a dramatic impact on worldwide health care systems that is determined by the growing prevalence of and the high exposure to cardiovascular and noncardiovascular events. Prognosis remains poor. We sought to compare a large population with HF across the ejection fraction (EF) spectrum with a population without HF for patient characteristics, and HF, cardiovascular, and noncardiovascular outcomes. Methods and Results Patients with HF registered in the Swedish HF registry in 2005 to 2018 were compared 1:3 with a sex-, age-, and county-matched population without HF. Outcomes were cardiovascular and noncardiovascular mortality and hospitalizations. Of 76 453 patients with HF, 53% had reduced EF, 23% mildly reduced EF, and 24% preserved EF. Compared with those without HF, patients with HF had more cardiovascular and noncardiovascular comorbidities and worse socioeconomic status. Incidence of cardiovascular and noncardiovascular events was higher in people with HF versus non-HF, with increased risk of all-cause (hazard ratio [HR], 2.53 [95% CI, 2.50-2.56]), cardiovascular (HR, 4.67 [95% CI, 4.59-4.76]), and noncardiovascular (HR, 1.49 [95% CI, 1.46-1.52]) mortality, 2- to 5-fold higher risk of first/repeated cardiovascular and noncardiovascular hospitalizations, and ~4 times longer in-hospital length of stay for any cause. Patients with HF with reduced EF had higher risk of HF hospitalizations, whereas those with HF with preserved EF had higher risk of all-cause and noncardiovascular hospitalization and mortality. Conclusions Patients with HF exert a high health care burden, with a much higher risk of cardiovascular, all-cause, and noncardiovascular events, and nearly 4 times as many days spent in hospital compared with those without HF. These epidemiological data may enable strategies for optimal resource allocation and HF trial design.
Keywords: comorbidity; ejection fraction; epidemiology; heart failure.
Figures
References
-
- Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, Allison M, Hemingway H, Cleland JG, McMurray JJV, et al. Temporal trends and patterns in heart failure incidence: a population‐based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5 - DOI - PMC - PubMed
-
- Moliner P, Lupon J, de Antonio M, Domingo M, Santiago‐Vacas E, Zamora E, Cediel G, Santesmases J, Diez‐Quevedo C, Troya MI, et al. Trends in modes of death in heart failure over the last two decades: less sudden death but cancer deaths on the rise. Eur J Heart Fail. 2019;21:1259–1266. doi: 10.1002/ejhf.1569 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
