

Implementation of the I-PASS handoff program in diverse clinical environments: A multicenter prospective effectiveness implementation study
- PMID: 36326255
- PMCID: PMC10964397
- DOI: 10.1002/jhm.12979
Implementation of the I-PASS handoff program in diverse clinical environments: A multicenter prospective effectiveness implementation study
Abstract
Background: Handoff miscommunications are a leading source of medical errors. Harmful medical errors decreased in pediatric academic hospitals following implementation of the I-PASS handoff improvement program. However, implementation across specialties has not been assessed.
Objective: To determine if I-PASS implementation across diverse settings would be associated with improvements in patient safety and communication.
Design: Prospective Type 2 Hybrid effectiveness implementation study.
Settings and participants: Residents from diverse specialties across 32 hospitals (12 community, 20 academic).
Intervention: External teams provided longitudinal coaching over 18 months to facilitate implementation of an enhanced I-PASS program and monthly metric reviews.
Main outcome and measures: Systematic surveillance surveys assessed rates of resident-reported adverse events. Validated direct observation tools measured verbal and written handoff quality.
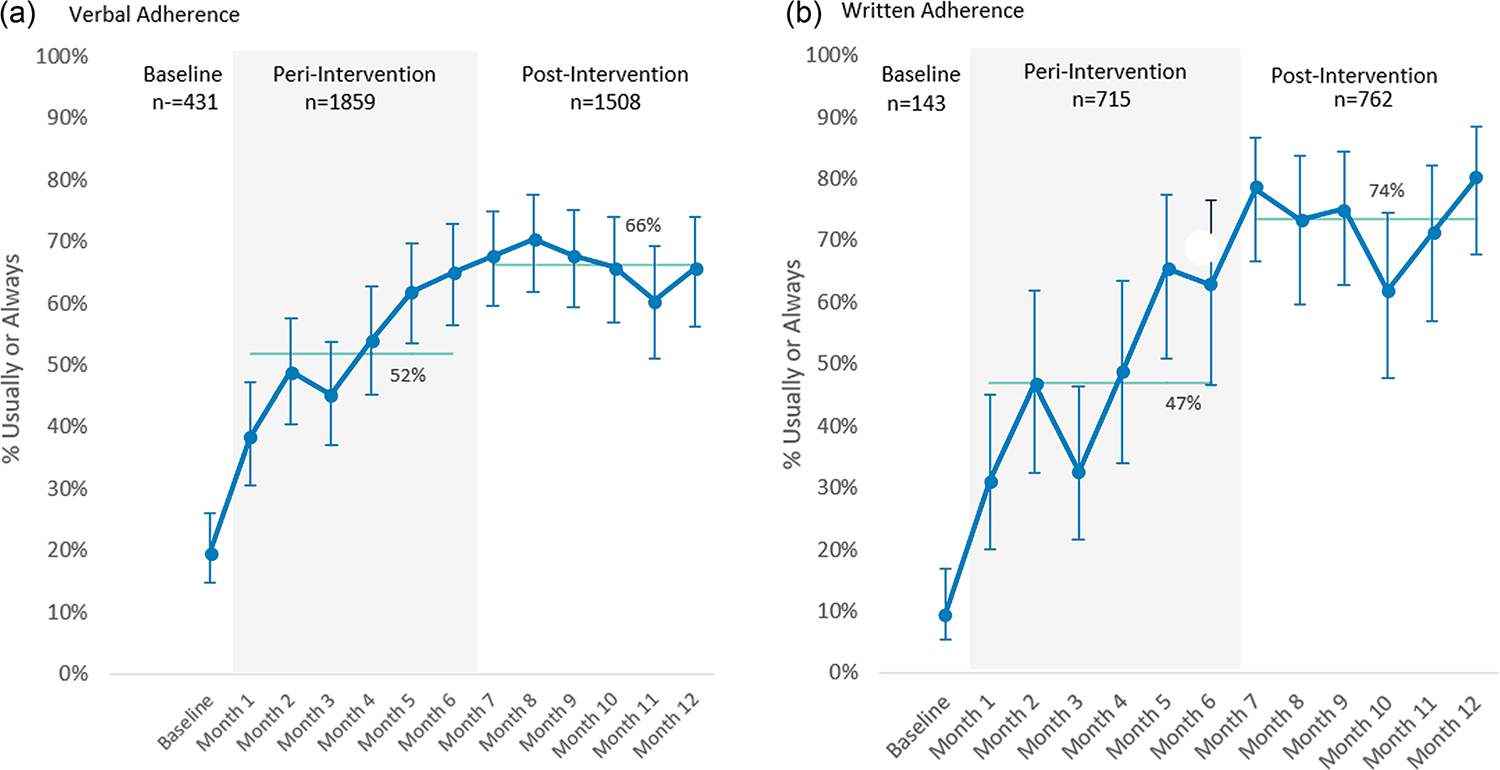
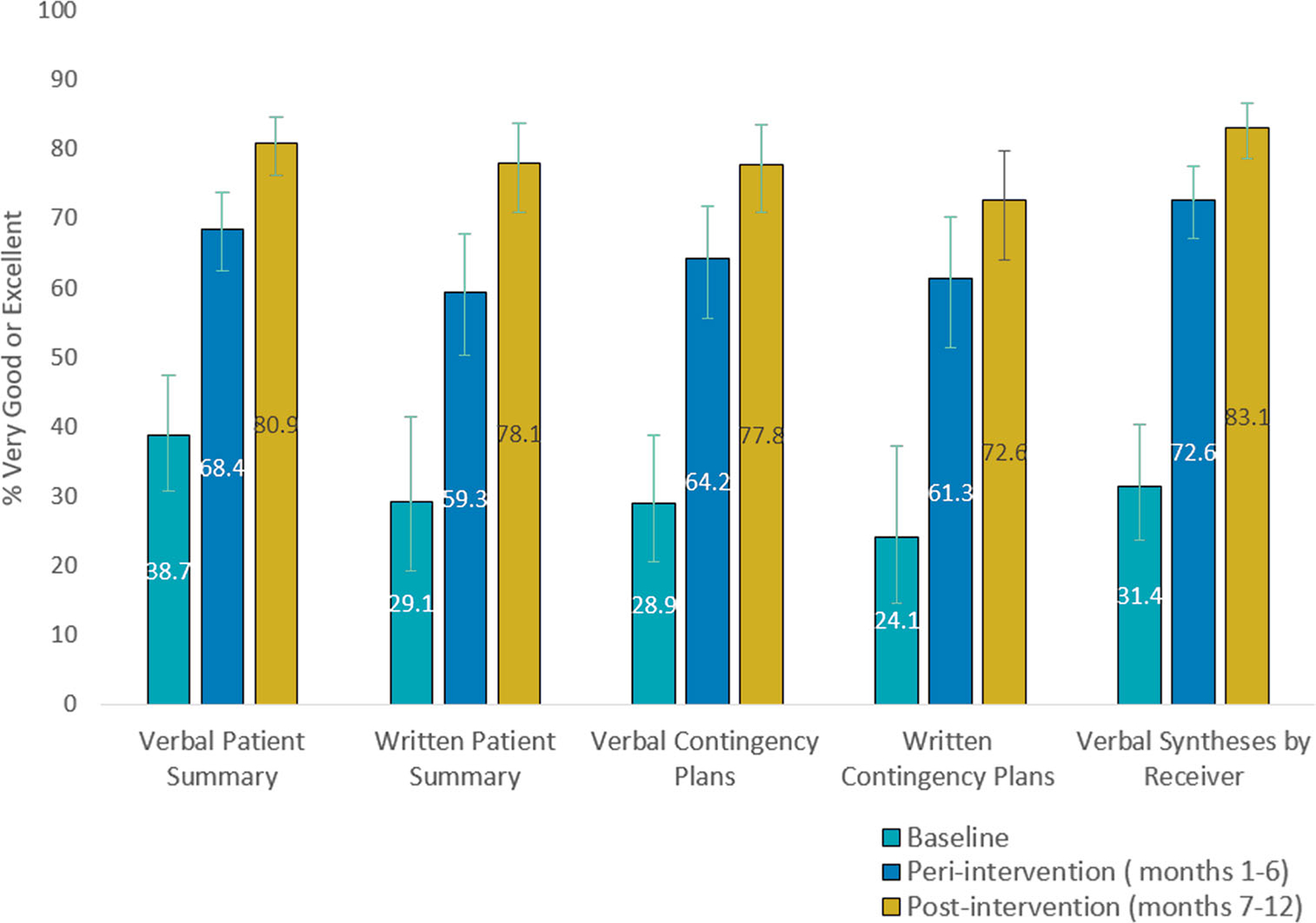
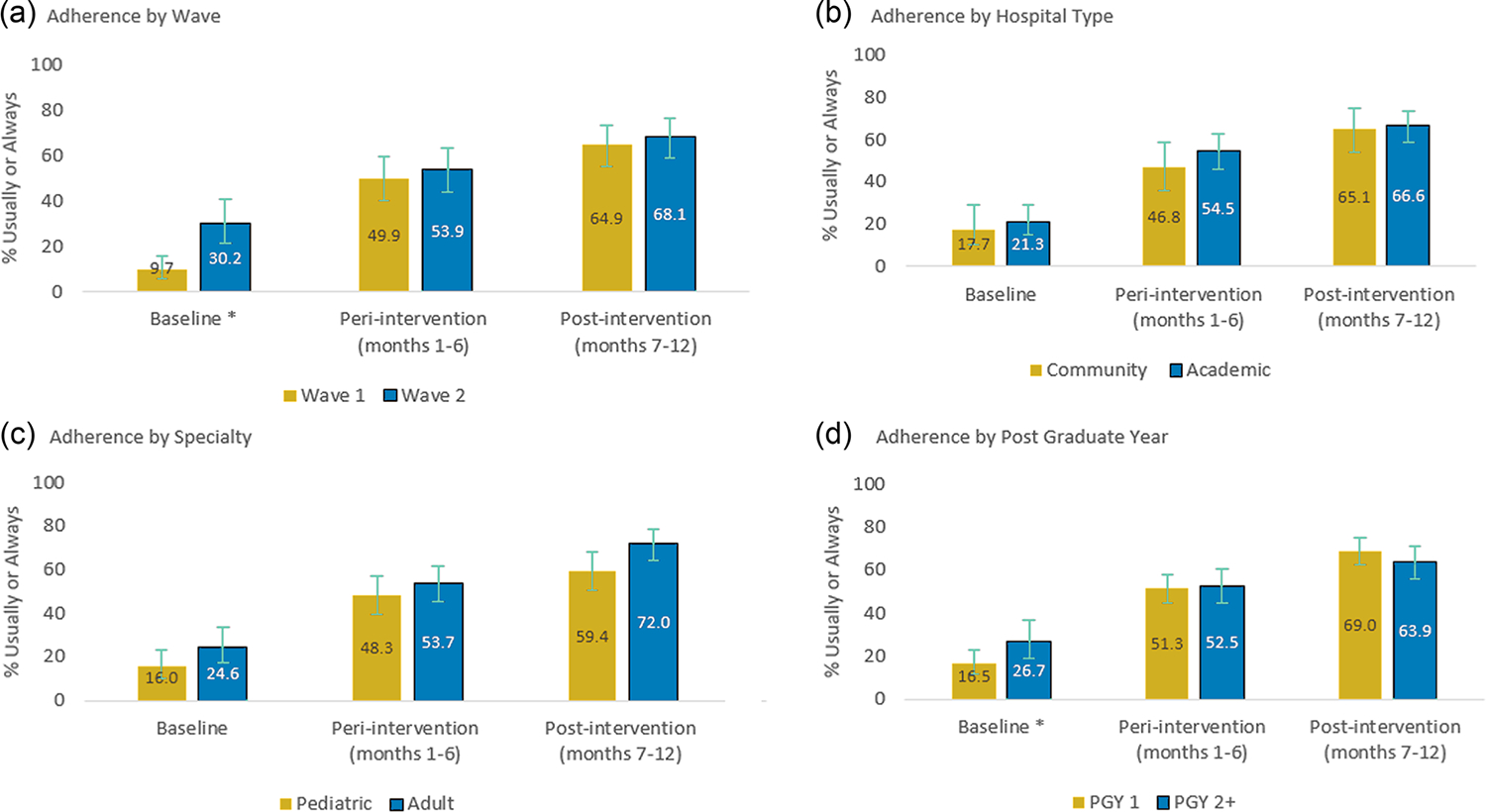
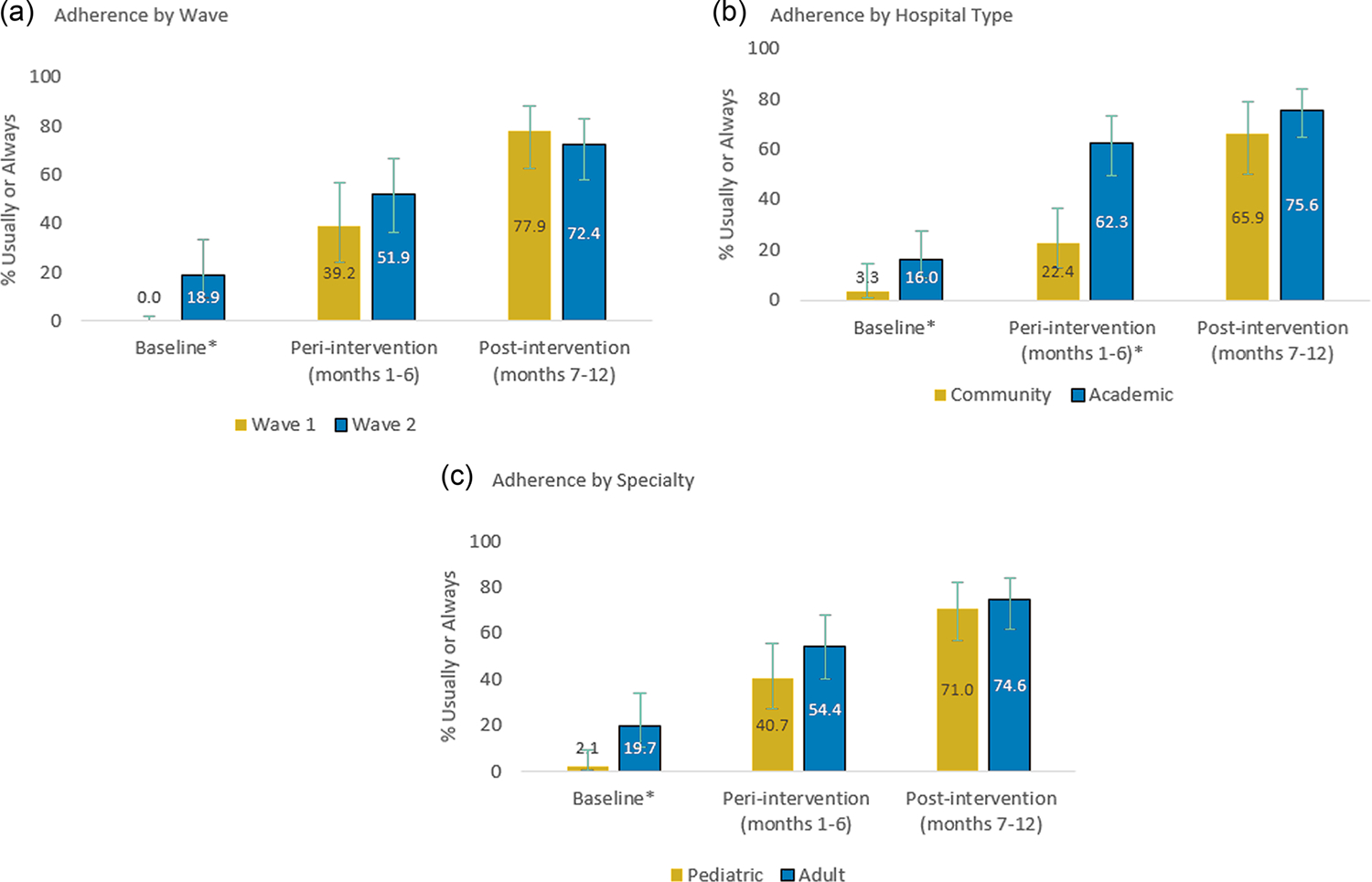
Results: 2735 resident physicians and 760 faculty champions from multiple specialties (16 internal medicine, 13 pediatric, 3 other) participated. 1942 error surveillance reports were collected. Major and minor handoff-related reported adverse events decreased 47% following implementation, from 1.7 to 0.9 major events/person-year (p < .05) and 17.5 to 9.3 minor events/person-year (p < .001). Implementation was associated with increased inclusion of all five key handoff data elements in verbal (20% vs. 66%, p < .001, n = 4812) and written (10% vs. 74%, p < .001, n = 1787) handoffs, as well as increased frequency of handoffs with high quality verbal (39% vs. 81% p < .001) and written (29% vs. 78%, p < .001) patient summaries, verbal (29% vs. 78%, p < .001) and written (24% vs. 73%, p < .001) contingency plans, and verbal receiver syntheses (31% vs. 83%, p < .001). Improvement was similar across provider types (adult vs. pediatric) and settings (community vs. academic).
© 2022 Society of Hospital Medicine.
Conflict of interest statement
CONFLICT OF INTEREST
All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- The Joint Commission. Sentinel event statistics released for 2014. The Joint Commission Online. Accessed October 6, 2017. http://www.jointcommission.org/assets/1/23/jconline_April_29_15.pdf
-
- Starmer AJ, Spector ND, West DC, Srivastava R, Sectish TC, Landrigan CP. Integrating research, quality improvement, and medical education for better handoffs and safer care: disseminating, adapting, and implementing the I-PASS program. Jt Comm J Qual Patient Saf. 2017;43(7):319–329. doi:10.1016/j.jcjq.2017.04.001 - DOI - PubMed
-
- Solet DJ, Norvell JM, Rutan GH, Frankel RM. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005;80(12):1094–1099. - PubMed
