

Interventions and outcomes of patients with multiple myeloma receiving salvage therapy after BCMA-directed CAR T therapy
- PMID: 36327160
- PMCID: PMC10082354
- DOI: 10.1182/blood.2022017848
Interventions and outcomes of patients with multiple myeloma receiving salvage therapy after BCMA-directed CAR T therapy
Abstract
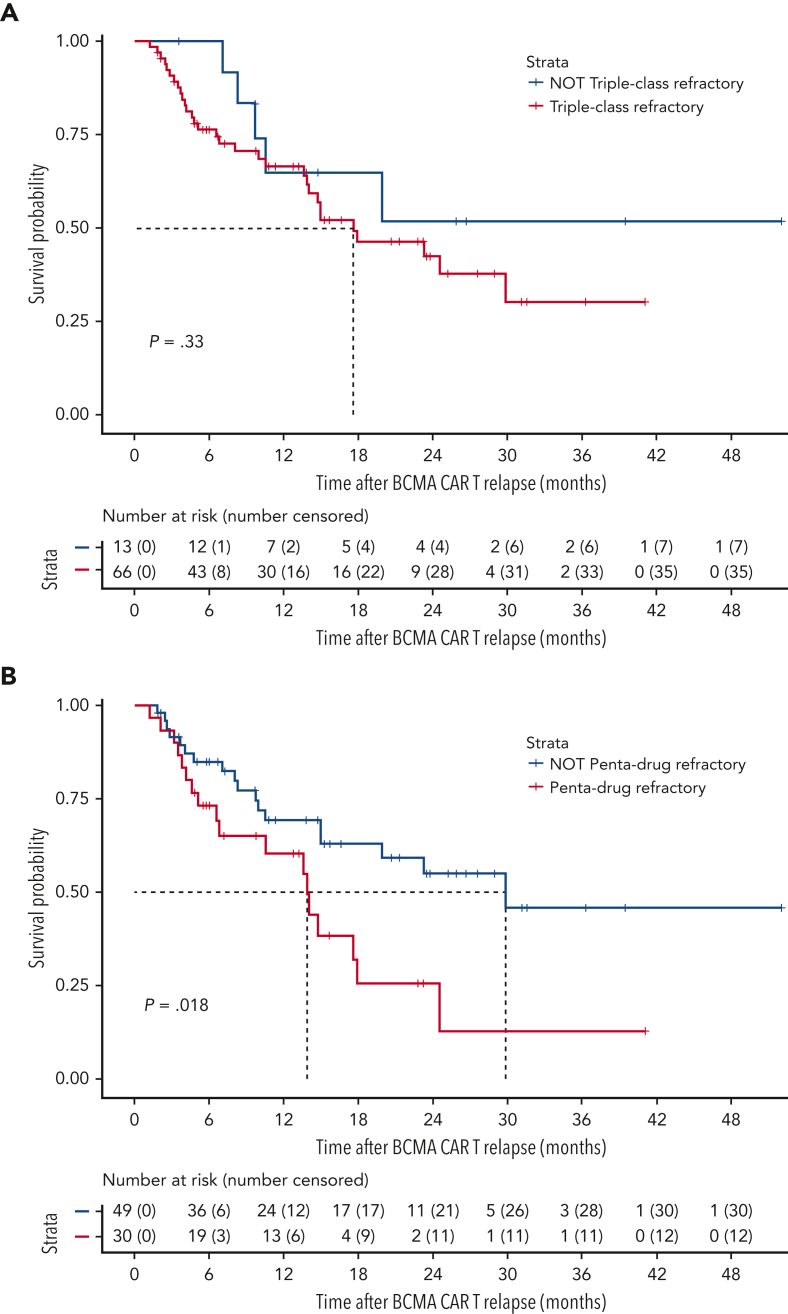
B-cell maturation antigen (BCMA)-directed chimeric antigen receptor T-cell (CAR T) therapy has demonstrated remarkable efficacy in patients with relapsed/refractory multiple myeloma, and now there are two US Food and Drug Administration-approved BCMA-directed CAR T products. However, despite high initial response rates, most patients eventually relapse. The outcomes of patients with disease recurrence after BCMA-directed CAR T have not been comprehensively studied, and such an analysis would help define optimal treatment strategies. We analyzed the salvage treatments and outcomes of 79 patients with multiple myeloma from two academic institutions, who had progression of disease after treatment with BCMA-directed CAR T. A total of 237 post-CAR T salvage treatment lines were used, and patients received a median of 2 (range, 1-10) treatment lines. The median overall survival from the date of relapse post-CAR T therapy was 17.9 months (95% confidence interval [CI], 14.0 non-estimable). The overall response rate to the first salvage regimen was 43.4%, with a median progression-free survival of 3.5 months (CI, 2.5-4.6). Thirty-five patients (44.3%) received a T-cell-engaging therapy (bispecific antibody or subsequent CAR T) as salvage treatment. The overall survival in patients who received subsequent T-cell-engaging therapy was not reached after a median follow up of 21.3 months. Patients with multiple myeloma who relapse after BCMA-directed CAR T have a limited prognosis but can be potentially treated with multiple lines of salvage therapy. T-cell-engaging therapies appear to maintain pronounced clinical activity in this setting.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: T.H.M. reports advisory board fees from Legend Biotech; G.L.S. receives research funding from Janssen, Amgen, and Beyond Spring; A.L. reports grant funding from Genmab, Amgen, Bristol Myers Squibb, and Janssen, has served on an advisory panel for Trillium Therapeutics, Pfizer, and Bristol Myers Squibb, and has received research funding from Janssen Oncology, Trillium Therapeutics, Genentech, Bristol Myers Squibb, Sanofi, and Pfizer; S.G. receives research funding from Miltenyi Biotec, Takeda Pharmaceutical, Celgene, Amgen, Sanofi, Johnson & Johnson, Actinium Pharmaceuticals, and Omeros, and is a member on the advisory boards for Kite Pharma, Celgene, Sanofi, Novartis, Johnson & Johnson, Amgen, Takeda Pharmaceutical, Jazz Pharmaceuticals, Janssen, Actinium Pharmaceuticals, and Spectrum Pharma; A.C. reports research support from Amgen, Array Biopharma, Celgene, GSK, Janssen, Millennium/Takeda, Novartis Pharmaceuticals, Oncoceutics, Pharmacyclics, and Seattle Genetics, consultancy fees from Amgen, Bristol Myers Squibb, Celgene, Millennium/Takeda, Janssen, and Karyopharm, and membership on the scientific advisory board for Amgen, Celgene, Millennium/Takeda, Janssen, Karyopharm, Sanofi, and Seattle Genetics; S.Z.U. reports grants/personal fees from Amgen, Celgene, Sanofi, Seattle Genetics, Janssen, Takeda, Skyline DX, Merck, and GSK, grant funding from BMS and Pharmacyclics; and personal fees from AbbVie, MundiPharma, Gilead, Genentech, and Oncopeptides; S.J. reports consulting fees for Bristol Myers Squibb (Celgene), Janssen, Karyopharm Therapeutics, Merck, Sanofi, and Takeda Pharmaceuticals; U.A.S. reports consultancy fees from Janssen, grant funding from the Parker Institute for Cancer Immunotherapy, the International Myeloma Society, Paula and Rodger Riney Foundation, Allen Foundation Inc, HealthTree Foundation, Janssen, Celgene/BMS, and the MSK Paul Calabresi Career Development Award for Clinical Oncology K12CA184746 and payment for lectures including service on speaker bureaus from ACCC and MJH Life Sciences; S.M. has received consulting fees from Evicore, Optum, BioAscend, Janssen Oncology, and Legend Biotech; T.F., G.L.S., A.L., S.G., S.U., U.A.S., and S.M. report funding support from the National Cancer Institute Memorial Sloan Kettering Core Grant (P30 CA008748); Memorial Sloan Kettering Cancer Center receives research funding from the National Cancer Institute, Janssen Oncology, Bristol Myers Squibb, Allogene Therapeutics, Fate Therapeutics, and Takeda Oncology for the research conducted by S.M. He has received honoraria from OncLive, Physician Education Resource, MJH Life Sciences, and Plexus Communications; S.P. is supported by NCI R01 CA244899, R01 CA252222, P30 CA196521 and research funding from Bristol Myers Squibb (Celgene), Karyopharm, and Amgen; The remaining authors declare no competing financial interests.
Figures



References
-
- Multiple myeloma . National Comprehensive Cancer Network (NCCN Guidelines®); 2022. Version 5.https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf - PubMed
-
- Munshi NC, Anderson LD, Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. - PubMed
-
- Berdeja JG, Madduri D, Usmani SZ, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. 2021;398(10297):314–324. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
