

Neural correlates linking trauma and physical symptoms
- PMID: 36327865
- PMCID: PMC9757618
- DOI: 10.1016/j.pscychresns.2022.111560
Neural correlates linking trauma and physical symptoms
Abstract
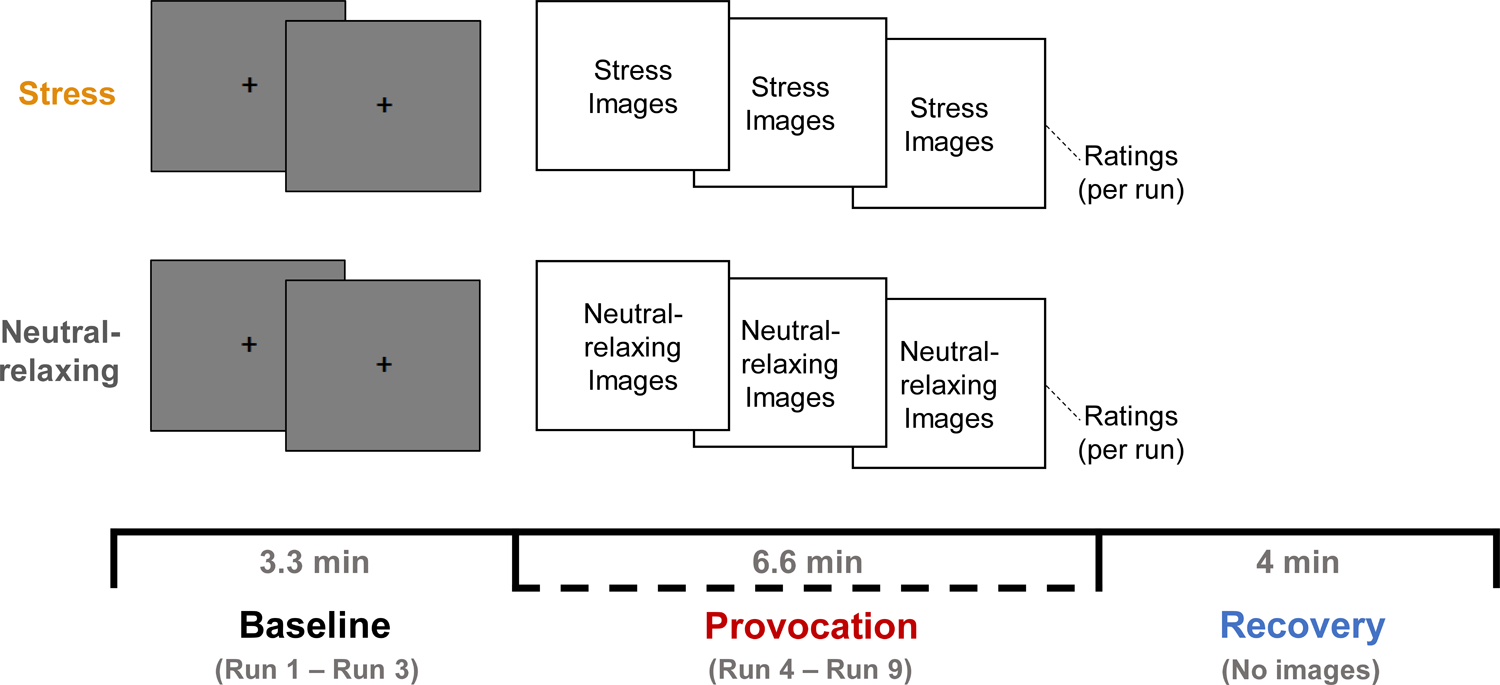
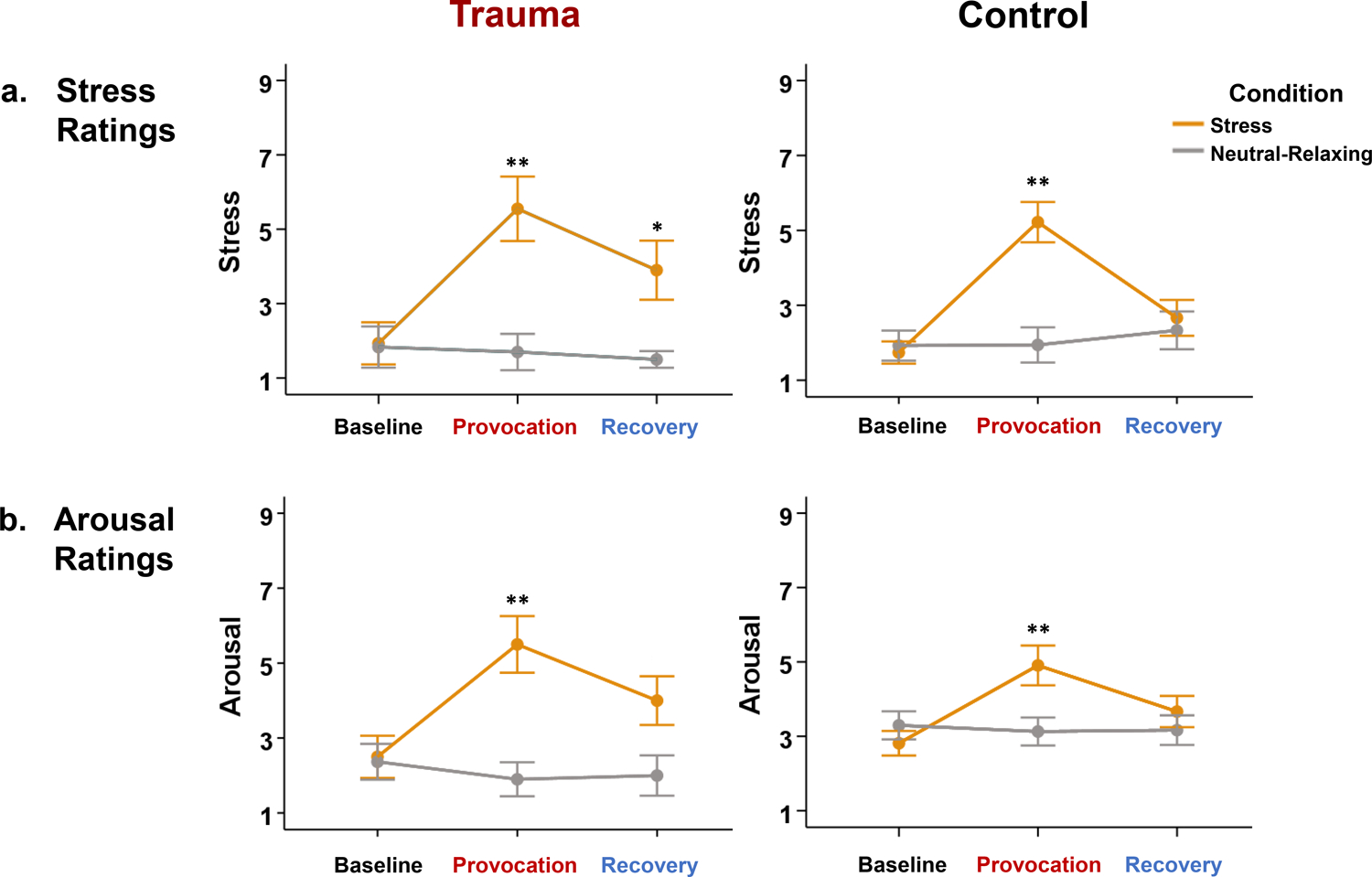
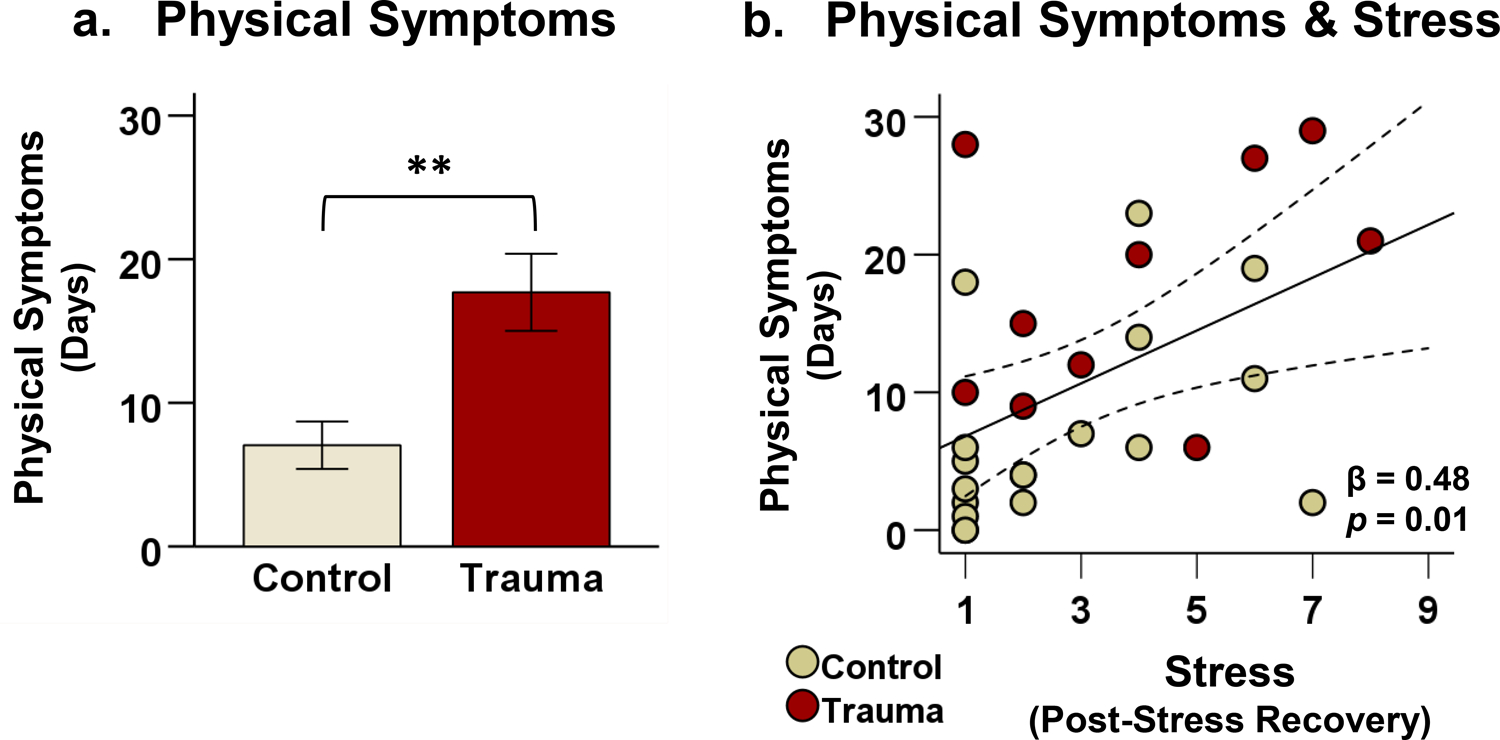
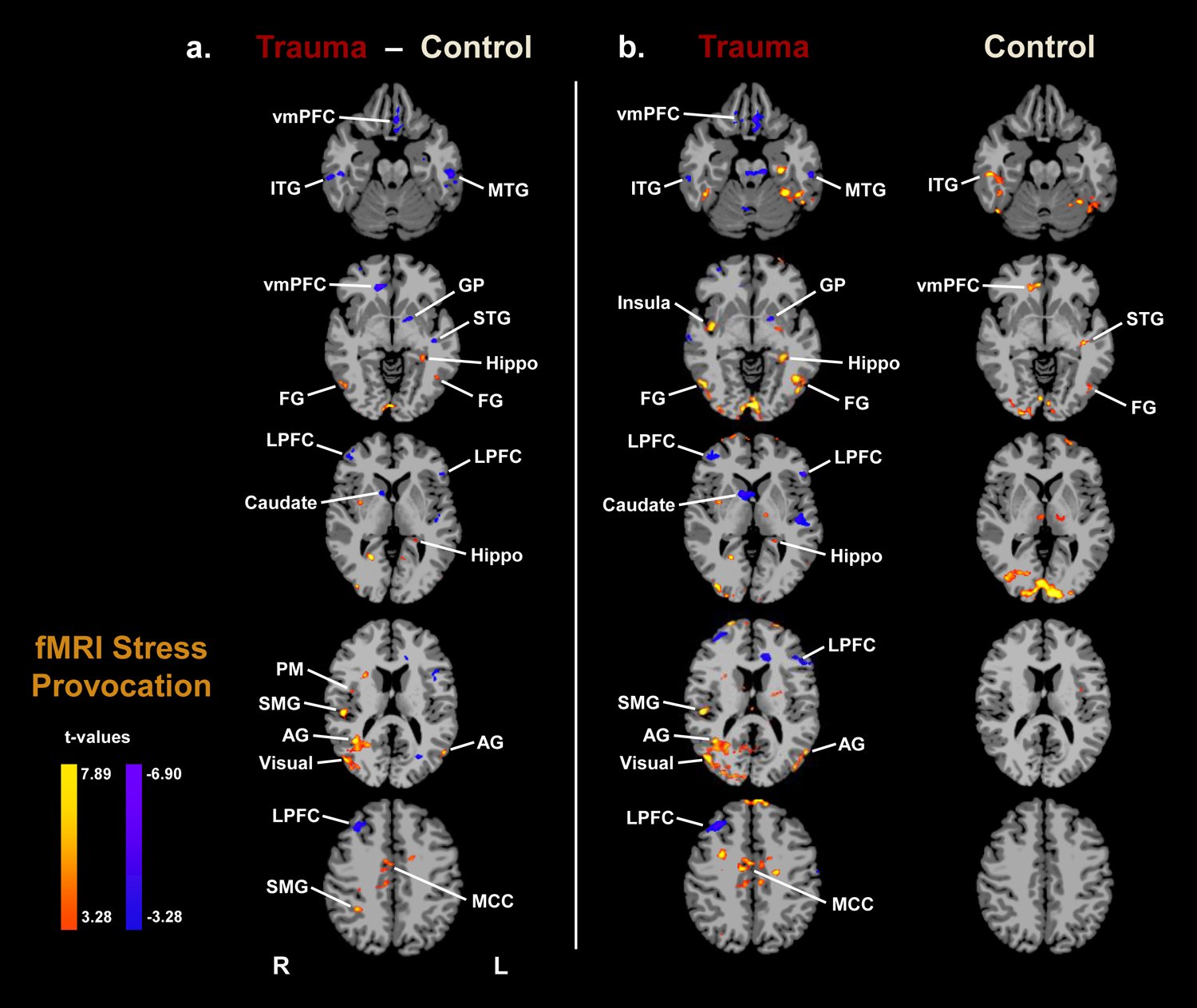
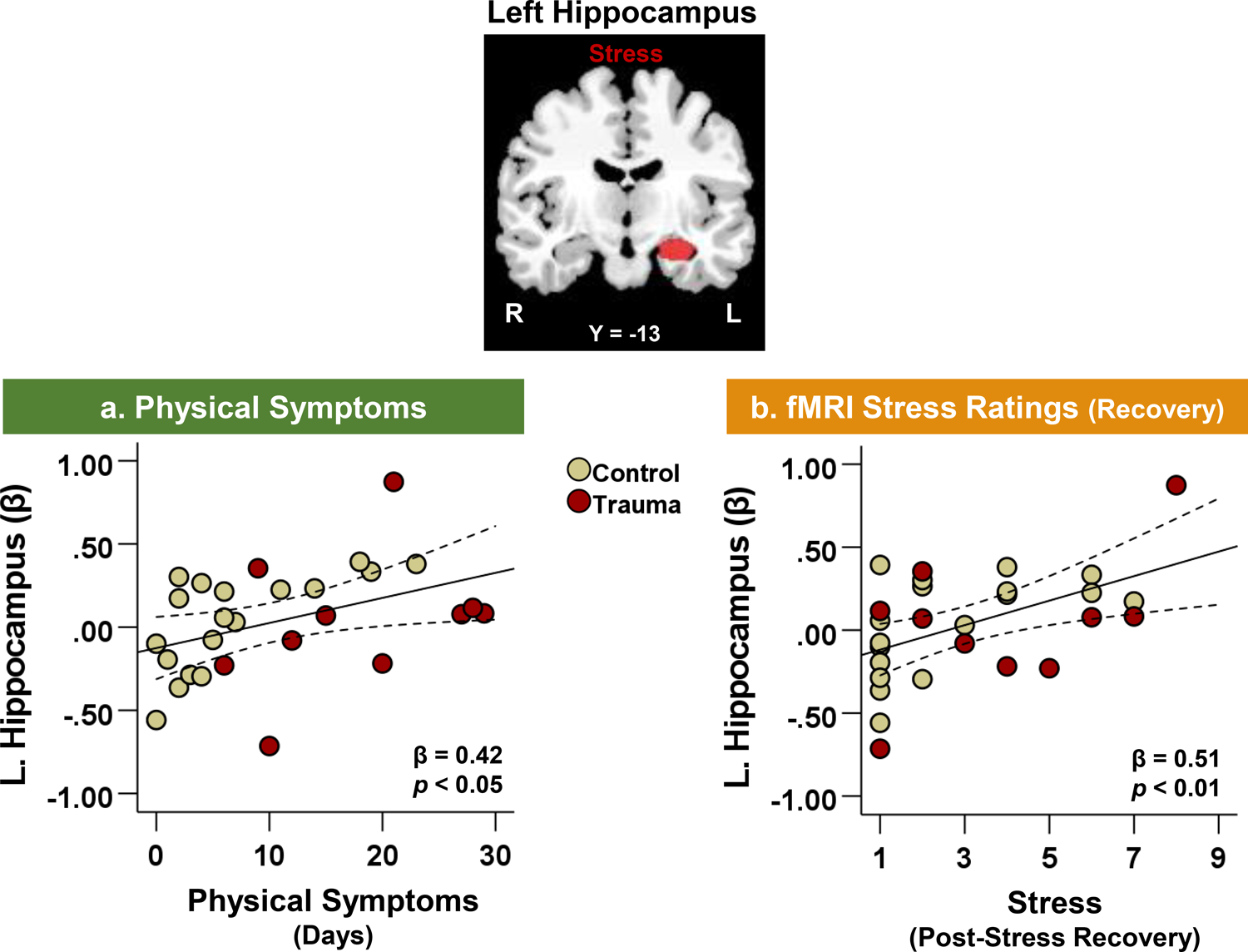
Trauma and chronic pain frequently co-occur, but the underlying neurological mechanisms are poorly understood. The current study investigated the neural correlates of stress and physical symptoms in trauma patients using functional magnetic resonance imaging (fMRI) and follow-up smartphone surveys. Participants were 10 patients diagnosed with Trauma- and Stressor-Related Disorders and 18 demographically-matched healthy controls who completed a fMRI stress provocation task in which they viewed stressful and neutral-relaxing images. Subsequently, participants completed daily smartphone surveys which prospectively monitored their stress and physical symptoms for 30 days. The trauma group experienced a significantly higher frequency of physical symptoms than controls during the follow-up period. During stress, trauma patients exhibited increased activity in the hippocampus, insula, and sensorimotor areas, but decreased activity in the ventromedial prefrontal cortex (vmPFC), lateral prefrontal cortex (LPFC), and dorsal striatum relative to controls. In all participants, higher physical symptom frequency was significantly associated with a hyperactive left hippocampal response to stress. The current study reports that trauma is characterized by greater physical symptoms and decreased prefrontal but increased limbic responses to stress. Our findings suggest that trauma may increase physical health symptoms by compromising hippocampal function, which could also increase vulnerability to stress- and pain-related disorders.
Keywords: Hippocampus; Pain; Physical symptoms; Stress; Trauma; fMRI.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest All authors declare no conflicts of interest or financial relationships with commercial interests.
Figures
References
-
- Agustin-Pavon C, Braesicke K, Shiba Y, Santangelo AM, Mikheenko Y, Cockroft G, Asma F, Clarke H, Man MS, & Roberts AC (2012). Lesions of ventrolateral prefrontal or anterior orbitofrontal cortex in primates heighten negative emotion. Biol Psychiatry, 72(4), 266–272. 10.1016/j.biopsych.2012.03.007 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
