

Elective surgery system strengthening: development, measurement, and validation of the surgical preparedness index across 1632 hospitals in 119 countries
- PMID: 36328042
- PMCID: PMC9621702
- DOI: 10.1016/S0140-6736(22)01846-3
Elective surgery system strengthening: development, measurement, and validation of the surgical preparedness index across 1632 hospitals in 119 countries
Abstract
Background: The 2015 Lancet Commission on global surgery identified surgery and anaesthesia as indispensable parts of holistic health-care systems. However, COVID-19 exposed the fragility of planned surgical services around the world, which have also been neglected in pandemic recovery planning. This study aimed to develop and validate a novel index to support local elective surgical system strengthening and address growing backlogs.
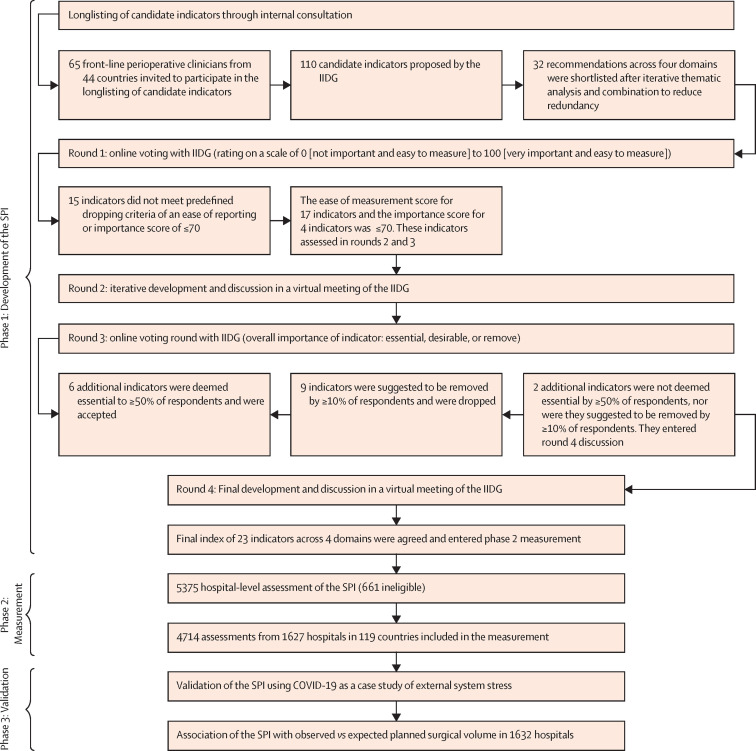
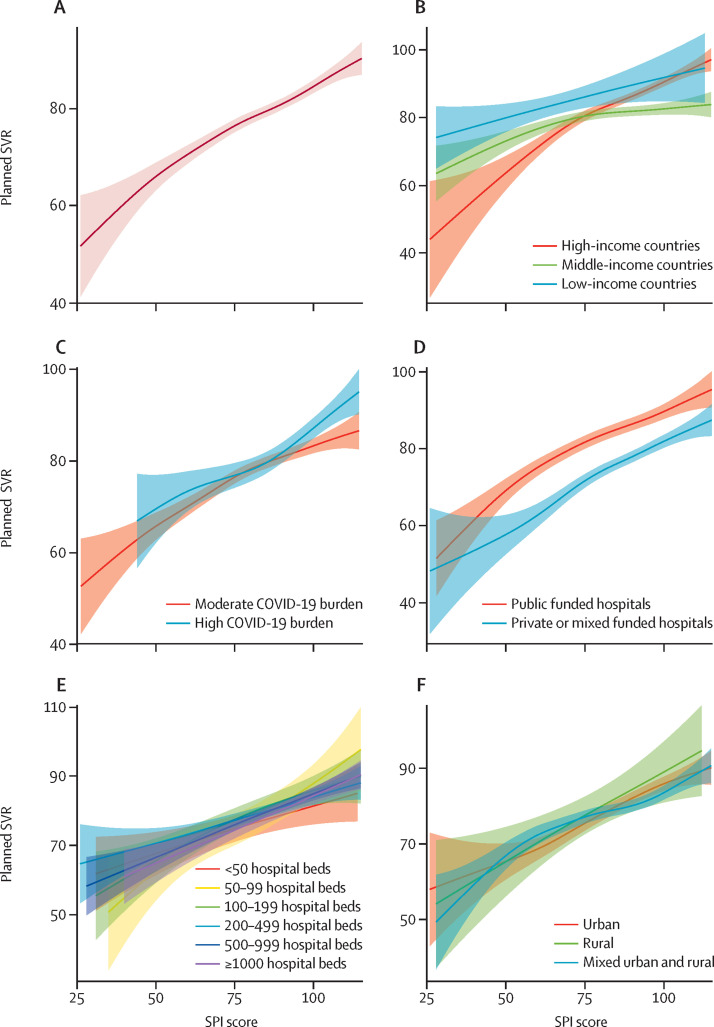
Methods: First, we performed an international consultation through a four-stage consensus process to develop a multidomain index for hospital-level assessment (surgical preparedness index; SPI). Second, we measured surgical preparedness across a global network of hospitals in high-income countries (HICs), middle-income countries (MICs), and low-income countries (LICs) to explore the distribution of the SPI at national, subnational, and hospital levels. Finally, using COVID-19 as an example of an external system shock, we compared hospitals' SPI to their planned surgical volume ratio (SVR; ie, operations for which the decision for surgery was made before hospital admission), calculated as the ratio of the observed surgical volume over a 1-month assessment period between June 6 and Aug 5, 2021, against the expected surgical volume based on hospital administrative data from the same period in 2019 (ie, a pre-pandemic baseline). A linear mixed-effects regression model was used to determine the effect of increasing SPI score.
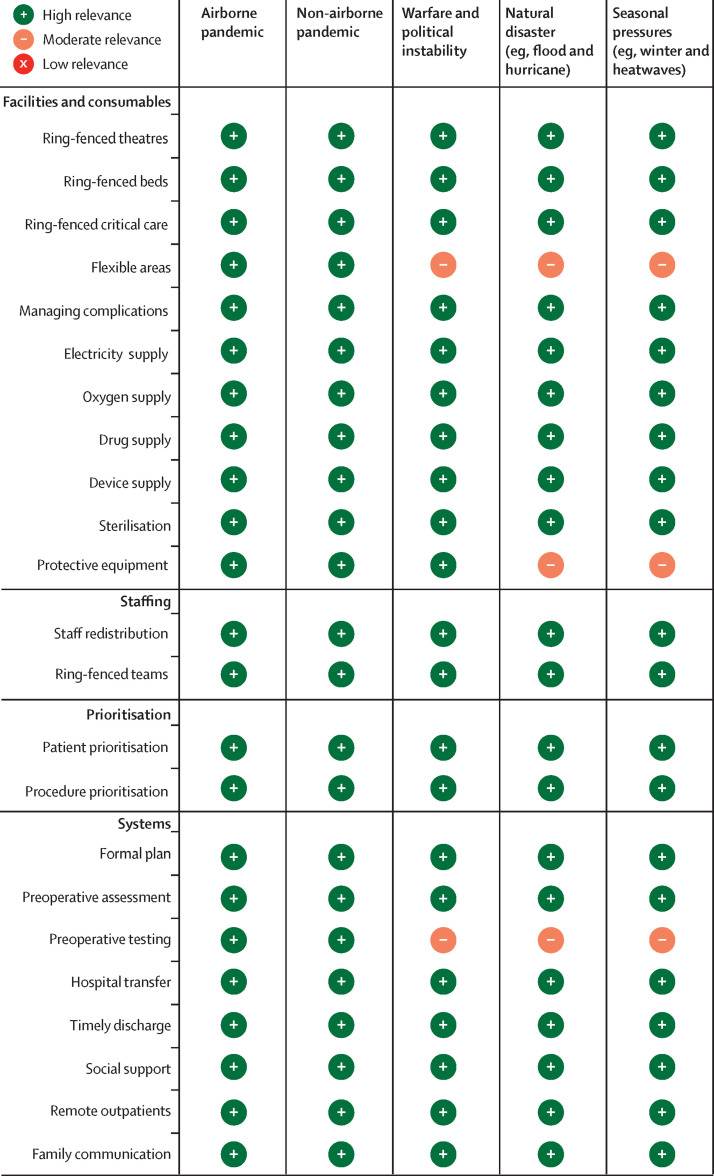
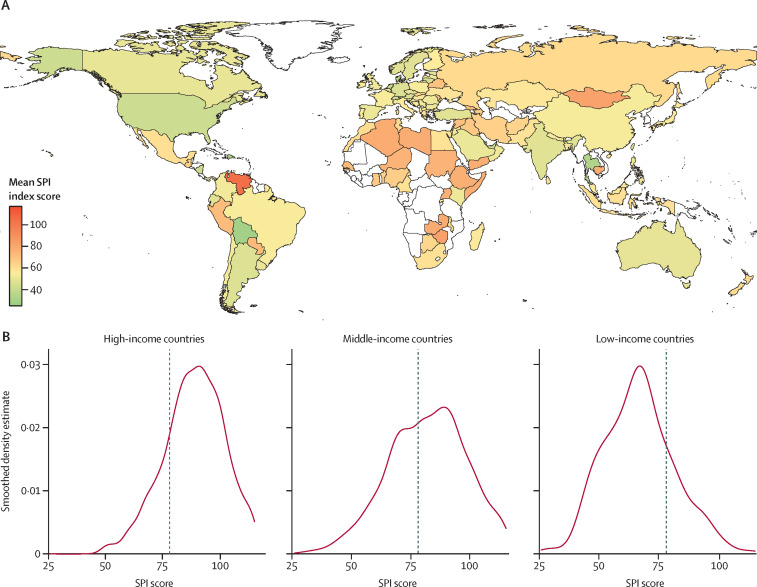
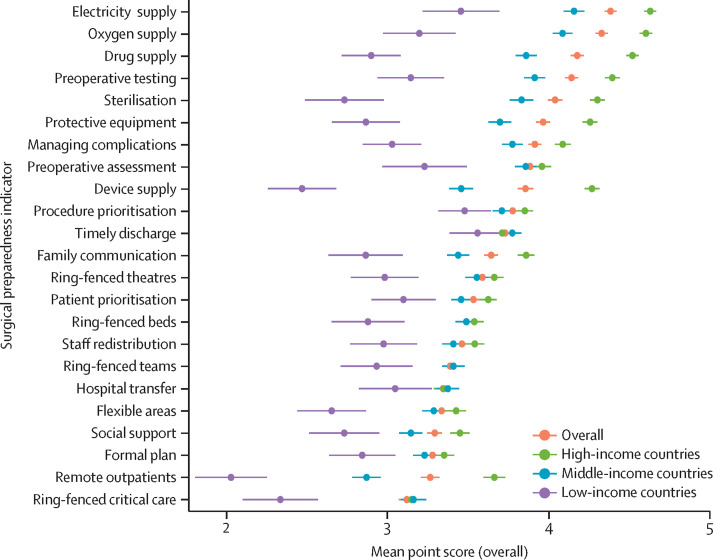
Findings: In the first phase, from a longlist of 103 candidate indicators, 23 were prioritised as core indicators of elective surgical system preparedness by 69 clinicians (23 [33%] women; 46 [67%] men; 41 from HICs, 22 from MICs, and six from LICs) from 32 countries. The multidomain SPI included 11 indicators on facilities and consumables, two on staffing, two on prioritisation, and eight on systems. Hospitals were scored from 23 (least prepared) to 115 points (most prepared). In the second phase, surgical preparedness was measured in 1632 hospitals by 4714 clinicians from 119 countries. 745 (45·6%) of 1632 hospitals were in MICs or LICs. The mean SPI score was 84·5 (95% CI 84·1-84·9), which varied between HIC (88·5 [89·0-88·0]), MIC (81·8 [82·5-81·1]), and LIC (66·8 [64·9-68·7]) settings. In the third phase, 1217 (74·6%) hospitals did not maintain their expected SVR during the COVID-19 pandemic, of which 625 (51·4%) were from HIC, 538 (44·2%) from MIC, and 54 (4·4%) from LIC settings. In the mixed-effects model, a 10-point increase in SPI corresponded to a 3·6% (95% CI 3·0-4·1; p<0·0001) increase in SVR. This was consistent in HIC (4·8% [4·1-5·5]; p<0·0001), MIC (2·8 [2·0-3·7]; p<0·0001), and LIC (3·8 [1·3-6·7%]; p<0·0001) settings.
Interpretation: The SPI contains 23 indicators that are globally applicable, relevant across different system stressors, vary at a subnational level, and are collectable by front-line teams. In the case study of COVID-19, a higher SPI was associated with an increased planned surgical volume ratio independent of country income status, COVID-19 burden, and hospital type. Hospitals should perform annual self-assessment of their surgical preparedness to identify areas that can be improved, create resilience in local surgical systems, and upscale capacity to address elective surgery backlogs.
Funding: National Institute for Health Research (NIHR) Global Health Research Unit on Global Surgery, NIHR Academy, Association of Coloproctology of Great Britain and Ireland, Bowel Research UK, British Association of Surgical Oncology, British Gynaecological Cancer Society, and Medtronic.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests RP has received research grants or consultancy fees or both from Edwards Lifesciences, Intersurgical, and GlaxoSmithKline. JM has consulted for WHO on projects related to perioperative preparedness. TA has received consultancy fees from MSD unrelated to this work. All other members of the writing group declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
- Archivio Istituzionale della Ricerca Unimi - Access Free Full Text
- Bern Open Repository and Information System
- ClinicalKey
- Elsevier Science
- Europe PubMed Central
- Linkoping University Electronic Press
- PubMed Central
- White Rose Research Online
- eScholarship, University of California - Access Free Full Text
Medical
