

Direct Oral Anticoagulants vs Vitamin K Antagonists in Patients With Antiphospholipid Syndromes: Meta-Analysis of Randomized Trials
- PMID: 36328154
- PMCID: PMC9812926
- DOI: 10.1016/j.jacc.2022.10.008
Direct Oral Anticoagulants vs Vitamin K Antagonists in Patients With Antiphospholipid Syndromes: Meta-Analysis of Randomized Trials
Abstract
Background: The efficacy and safety of direct oral anticoagulants (DOACs) for patients with thrombotic antiphospholipid syndrome remain controversial.
Objectives: The authors performed a systematic review and meta-analysis of randomized controlled trials that compared DOACs with vitamin K antagonists (VKAs).
Methods: We searched PubMed, EMBASE, and Cochrane Central Register of Controlled Trials through April 9, 2022. The 2 main efficacy outcomes were a composite of arterial thrombotic events and venous thromboembolic events (VTEs). The main safety outcome was major bleeding. Random effects models with inverse variance were used.
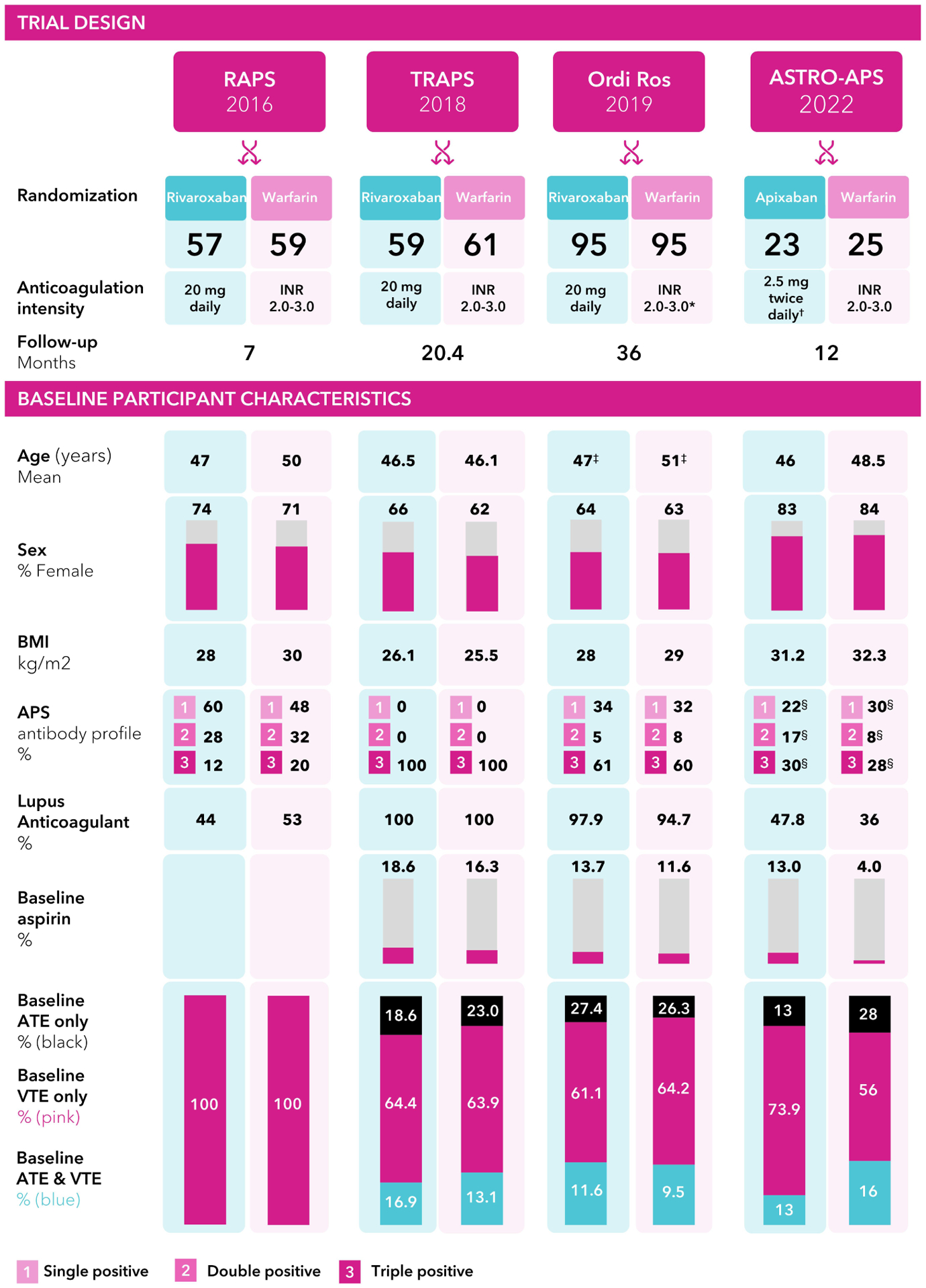
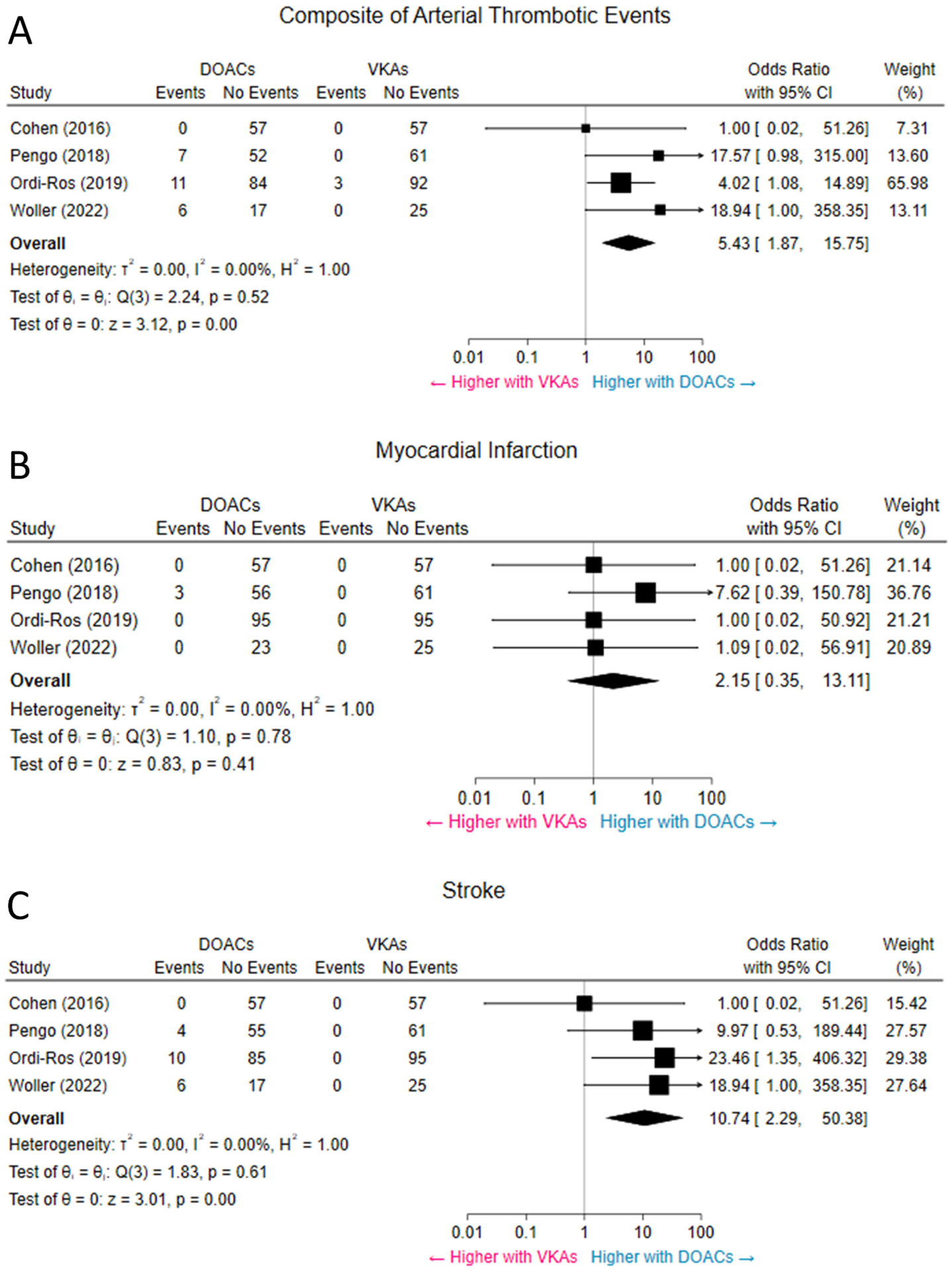
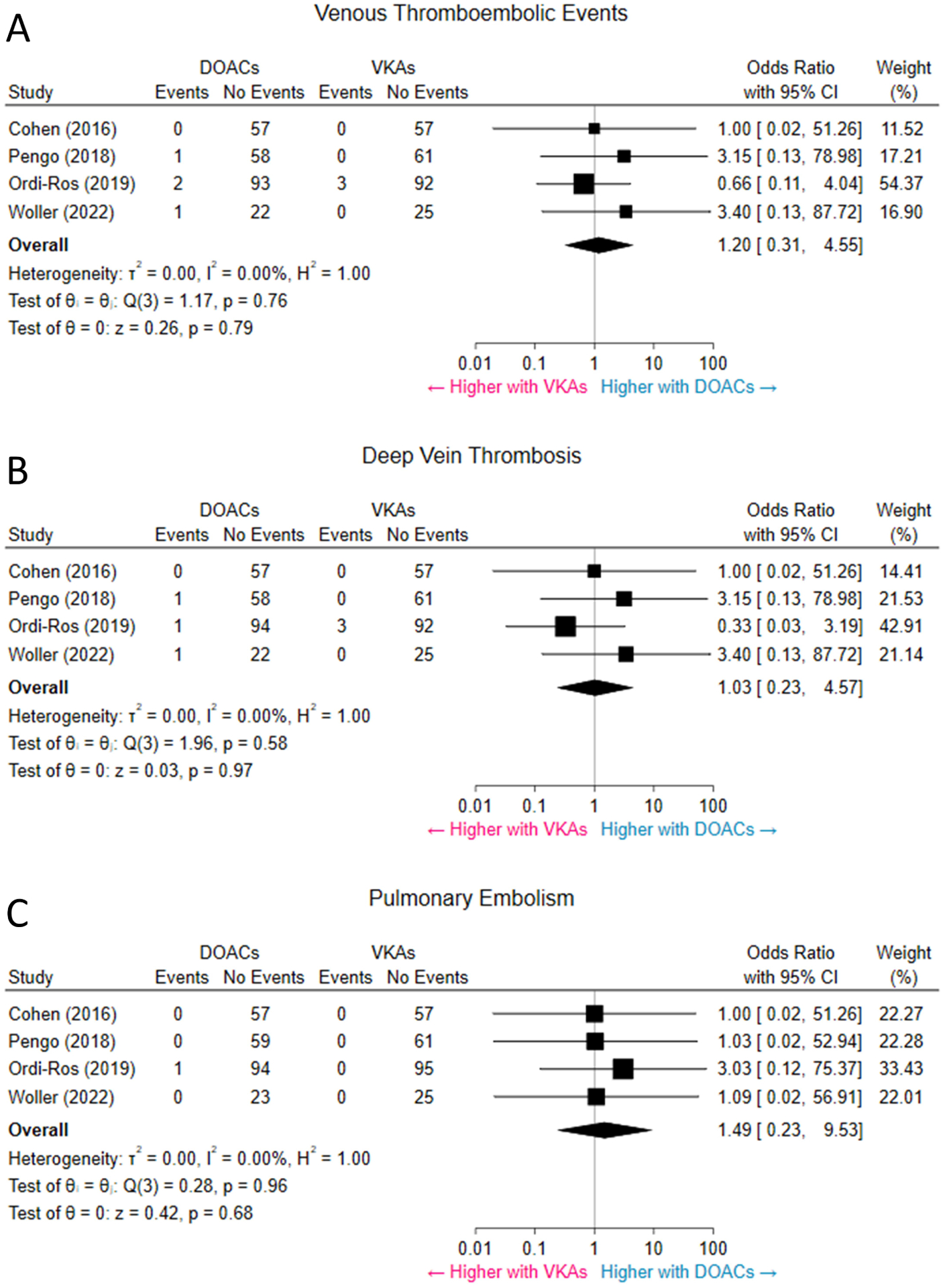
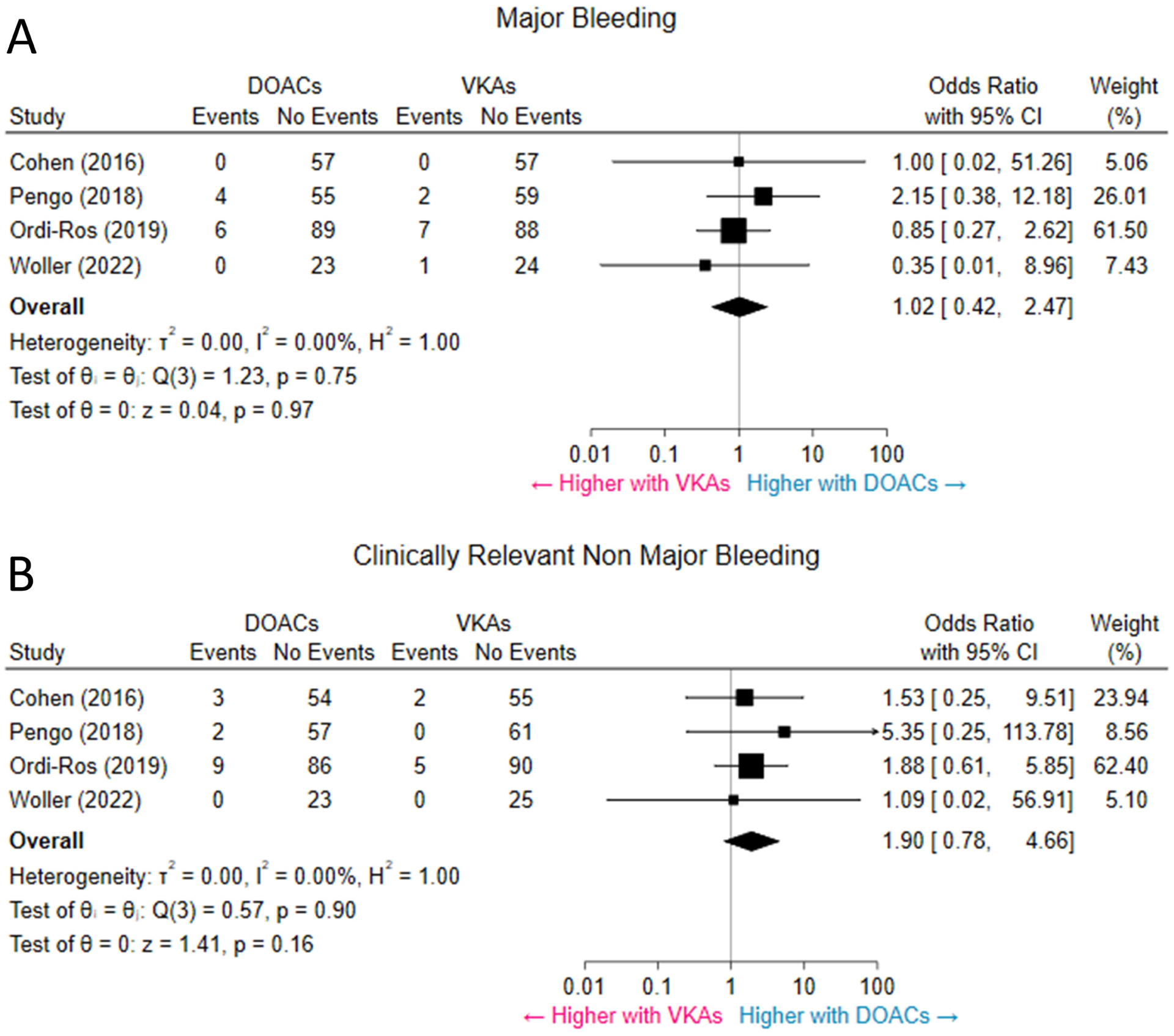
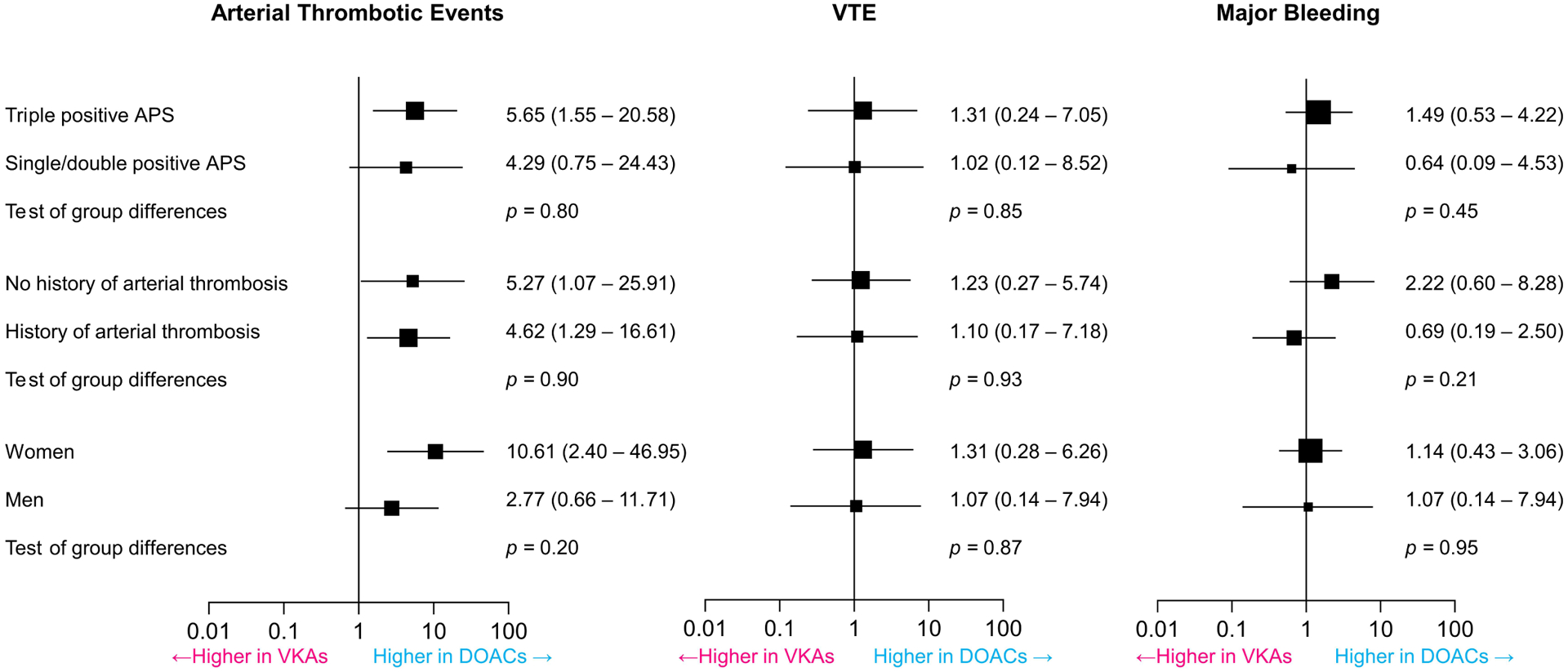
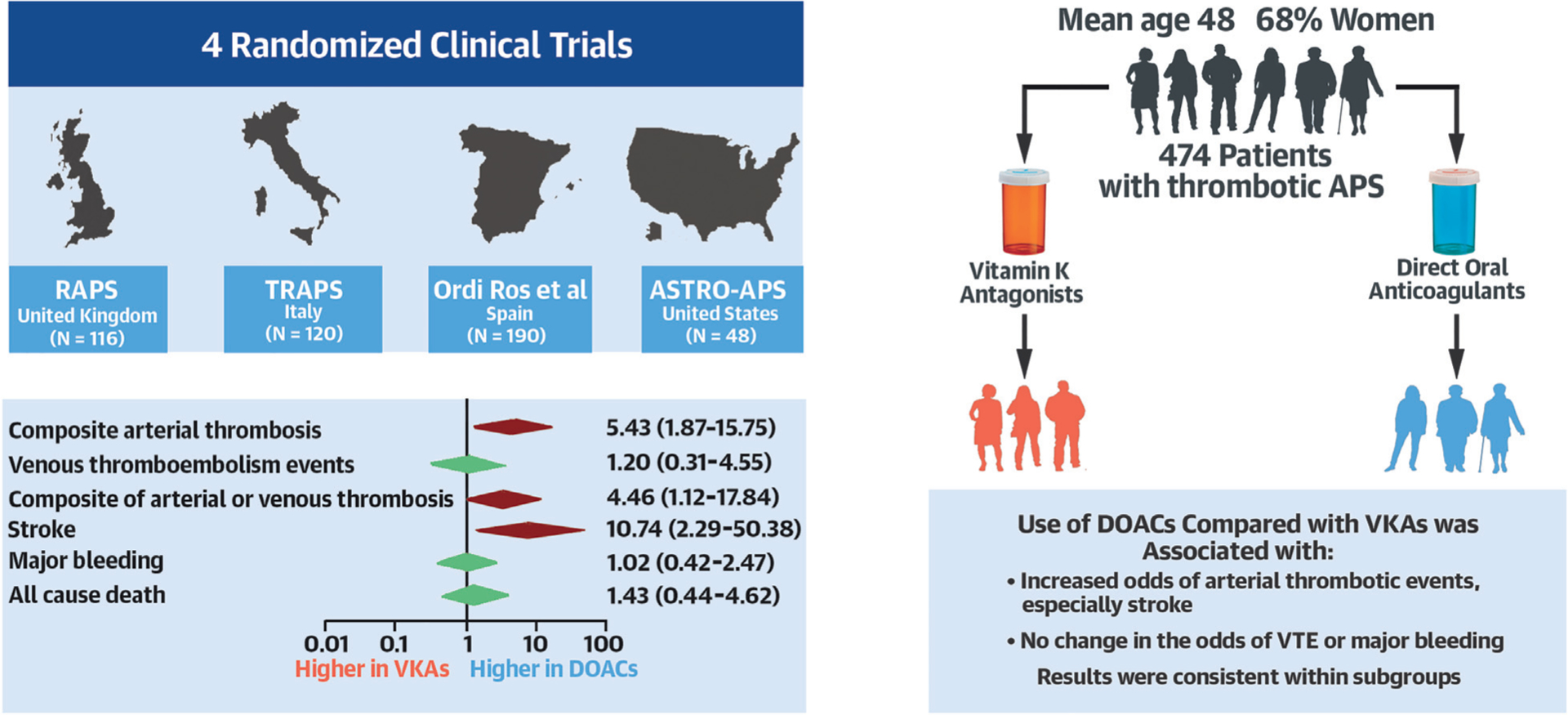
Results: Our search retrieved 253 studies. Four open-label randomized controlled trials involving 472 patients were included (mean control-arm time-in-therapeutic-range 60%). All had proper random sequence generation and adequate allocation concealment. Overall, the use of DOACs compared with VKAs was associated with increased odds of subsequent arterial thrombotic events (OR: 5.43; 95% CI: 1.87-15.75; P < 0.001, I2 = 0%), especially stroke, and the composite of arterial thrombotic events or VTE (OR: 4.46; 95% CI: 1.12-17.84; P = 0.03, I2 = 0%). The odds of subsequent VTE (OR: 1.20; 95% CI: 0.31-4.55; P = 0.79, I2 = 0%), or major bleeding (OR: 1.02; 95% CI: 0.42-2.47; P = 0.97; I2 = 0%) were not significantly different between the 2 groups. Most findings were consistent within subgroups.
Conclusions: Patients with thrombotic antiphospholipid syndrome randomized to DOACs compared with VKAs appear to have increased risk for arterial thrombosis. No significant differences were observed between patients randomized to DOACs vs VKAs in the risk of subsequent VTE or major bleeding.
Keywords: arterial thrombosis; bleeding; mortality; stroke; venous thromboembolism.
Copyright © 2023 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Piazza has received research support from Bristol Myers Squibb/Pfizer Alliance, Bayer, Janssen, Alexion, Amgen, and Boston Scientific Corporation; and has received consulting fees from Bristol Myers Squibb/Pfizer Alliance, Boston Scientific Corporation, Janssen, Namsa, Prairie Education and Research Cooperative, Boston Clinical Research Institute, and Amgen. Dr Jiménez has received research support from Daiichi-Sankyo and Sanofi; and has received consulting fees from Bristol Myers Squibb/Pfizer Alliance, Daiichi-Sankyo, Leo Pharma, Rovi, and Sanofi. Dr Monreal has received research support from Sanofi, Leo, and Rovi; and has received consulting fees from Sanofi. Dr Pengo has received lecture fees from Werfen Group. Dr Cortes-Hernandez has received institutional research funding from Bayer Hispania to conduct the APS RCT. Dr Connors has received research funding to her institution from CSL Behring; has received consulting fees from Abbott; has received honoraria for lectures from Bristol Myers Squibb, Roche, and Sanofi; and has participated on the advisory board of Abbott, Alnylam, Anthos, Bristol Myers Squibb, Sanofi, and Takeda, outside of the submitted work. Dr Kanthi is an inventor on a pending patent application by the University of Michigan on the use of biogases in vascular disease (US202201670756A1); and is supported by the National Heart, Lung, and Blood Institute Intramural Research Program and the Lasker Foundation. Dr Krumholz has received (within the last 3 years) expenses and/or personal fees from UnitedHealth, Element Science, Aetna, Reality Labs, Tesseract/4Catalyst, F-Prime, the Siegfried and Jensen Law Firm, the Arnold and Porter Law Firm, and the Martin/Baughman Law Firm; is a cofounder of Refactor Health, an enterprise health care artificial intelligence–augmented data management company, and HugoHealth, a personal health information platform; and is associated with contracts through Yale University from Johnson and Johnson. Dr Middeldorp has received grants and personal fees from Daiichi-Sankyo; has received grants and personal fees from Bayer, Pfizer, and Boehringer Ingelheim; and has received personal fees from Portola/Alexion, Abbvie, Bristol Myers Squibb Pfizer, Norgine, and Viatris, all paid to her institution. Dr Falanga has received honoraria/consulting fees from Stago, Sanofi, Daiichi-Sankyo, Leo Pharma, and Pfizer. Dr Goldhaber has received research support from Bayer, Bristol Myers Squibb, Boston Scientific BTG EKOS, Janssen, National Heart, Lung, and Blood Institute, and Pfizer; and has received consulting fees from Agile, Bayer, and Pfizer. Dr Bikdeli is a consulting expert, on behalf of the plaintiff, for litigation related to 2 specific brand models of IVC filters; and is supported by the Scott Schoen and Nancy Adams IGNITE Award from the Mary Horrigan Connors Center for Women's Health and Gender Biology at Brigham and Women's Hospital and a Career Development Award from the American Heart Association and VIVA Physicians (#938814). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Warfarin Is the Preferred Therapy for Patients With Thrombotic APS: Back to the Future.J Am Coll Cardiol. 2023 Jan 3;81(1):31-33. doi: 10.1016/j.jacc.2022.10.015. Epub 2022 Oct 31. J Am Coll Cardiol. 2023. PMID: 36328156 No abstract available.
-
In thrombotic antiphospholipid syndrome, DOACs vs. VKAs increase arterial thrombotic events but not major bleeding.Ann Intern Med. 2023 Apr;176(4):JC43. doi: 10.7326/J23-0016. Epub 2023 Apr 4. Ann Intern Med. 2023. PMID: 37011391
References
-
- Garcia D, Erkan D. Diagnosis and Management of the Antiphospholipid Syndrome. N Engl J Med 2018;378:2010–2021. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51. - PubMed
-
- Agnelli G, Buller HR, Cohen A et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med 2013;368:699–708. - PubMed
-
- Investigators E, Bauersachs R, Berkowitz SD et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010;363:2499–510. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
