

Oxalate homeostasis
- PMID: 36329260
- PMCID: PMC10278040
- DOI: 10.1038/s41581-022-00643-3
Oxalate homeostasis
Abstract
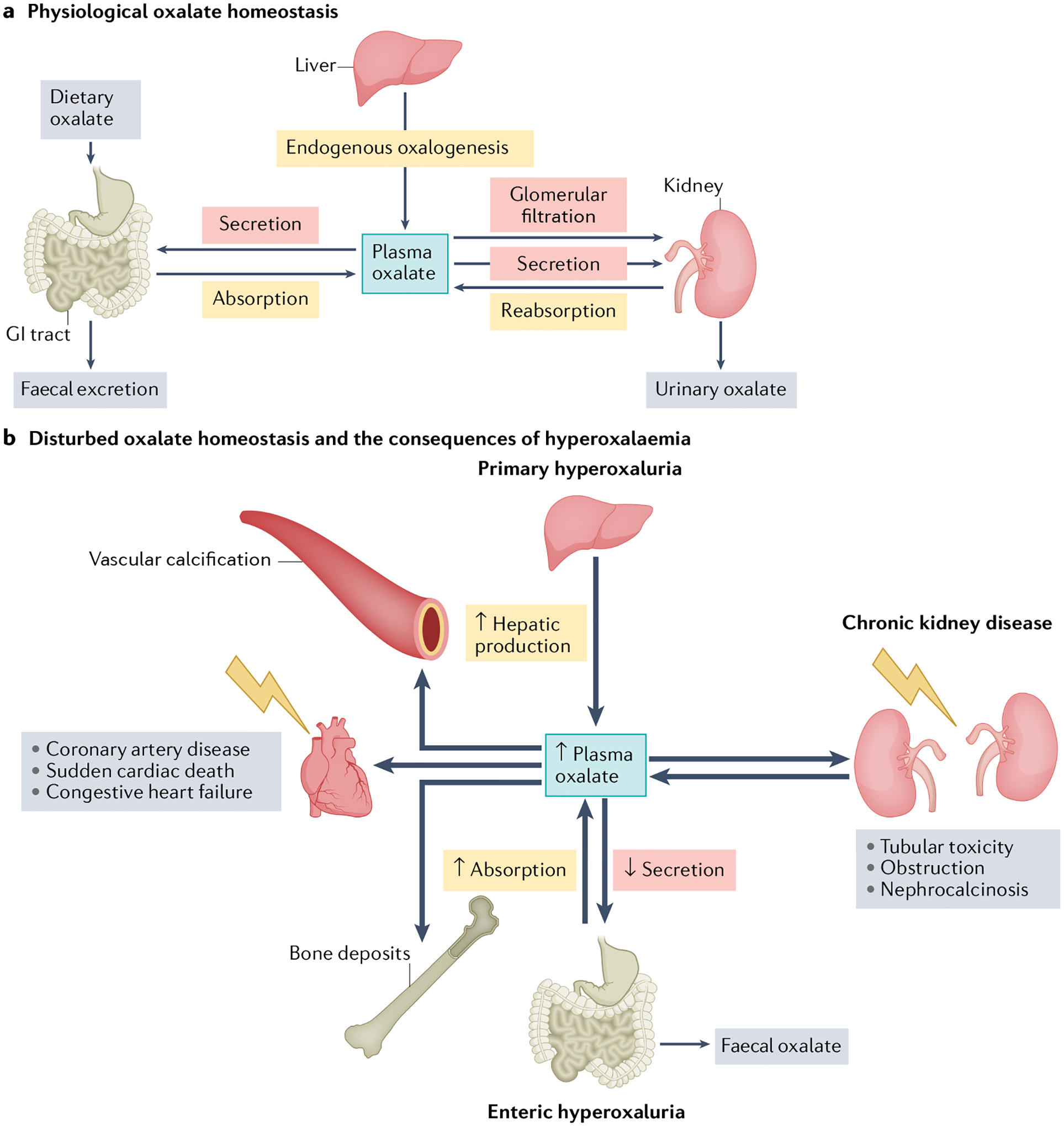
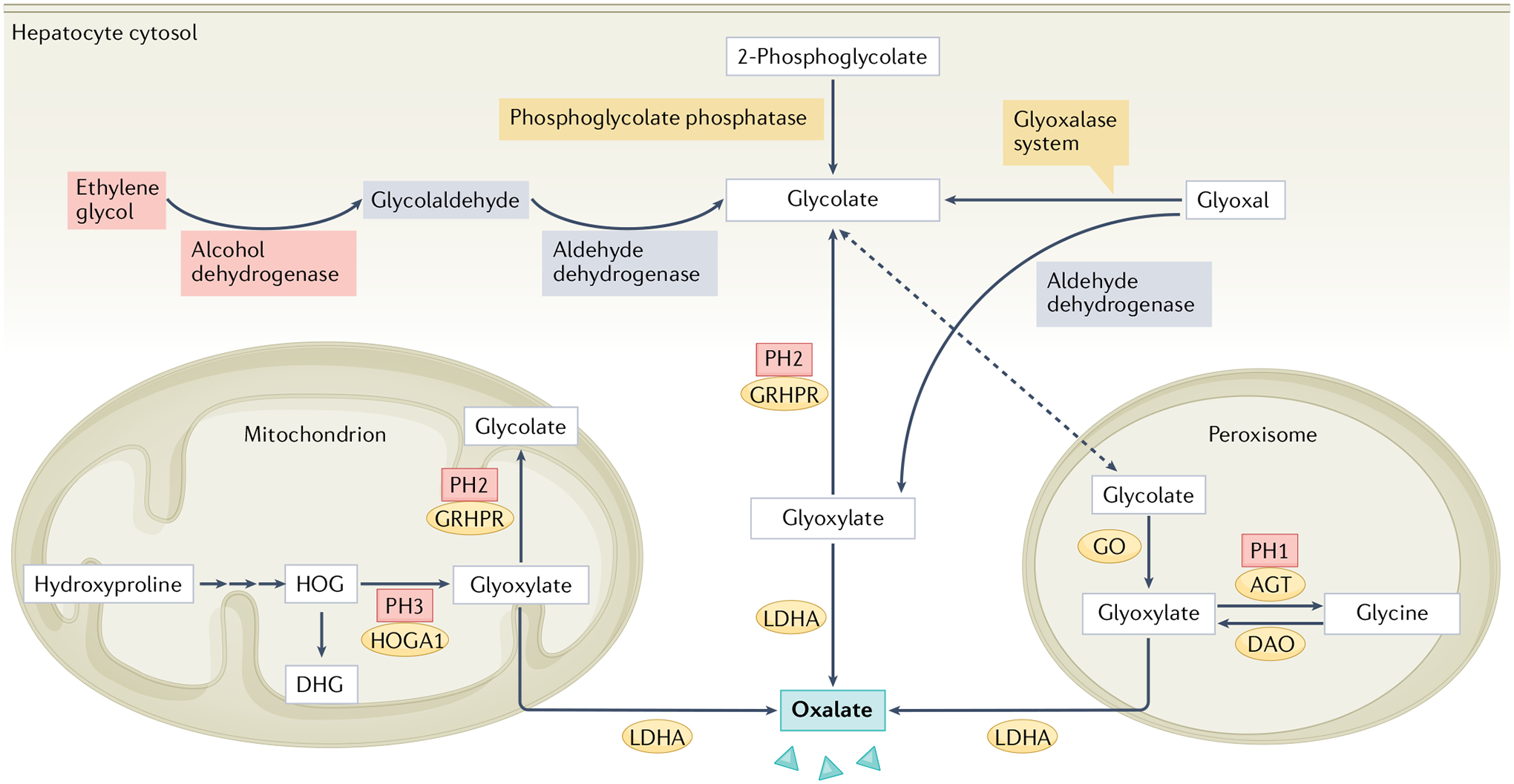
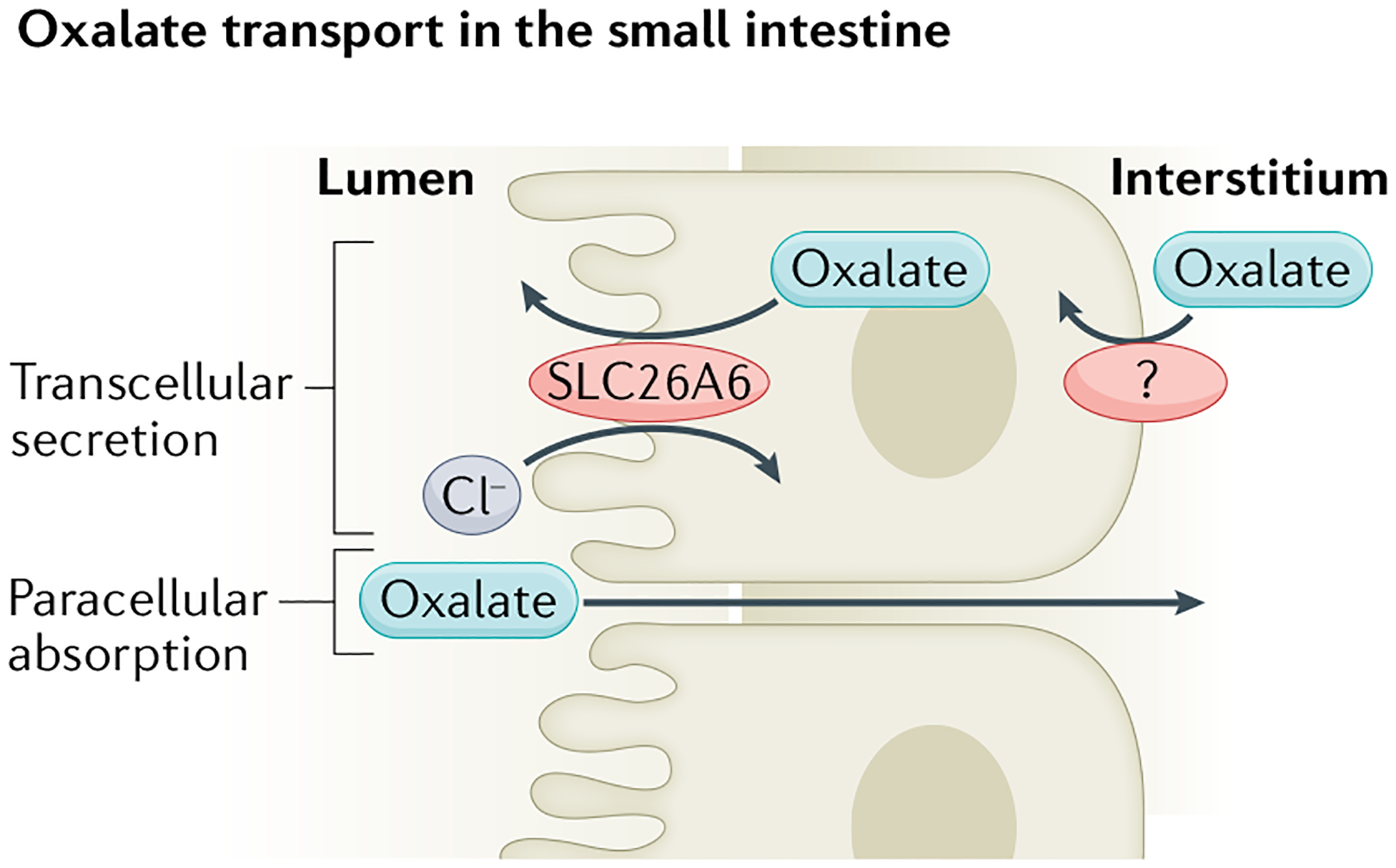
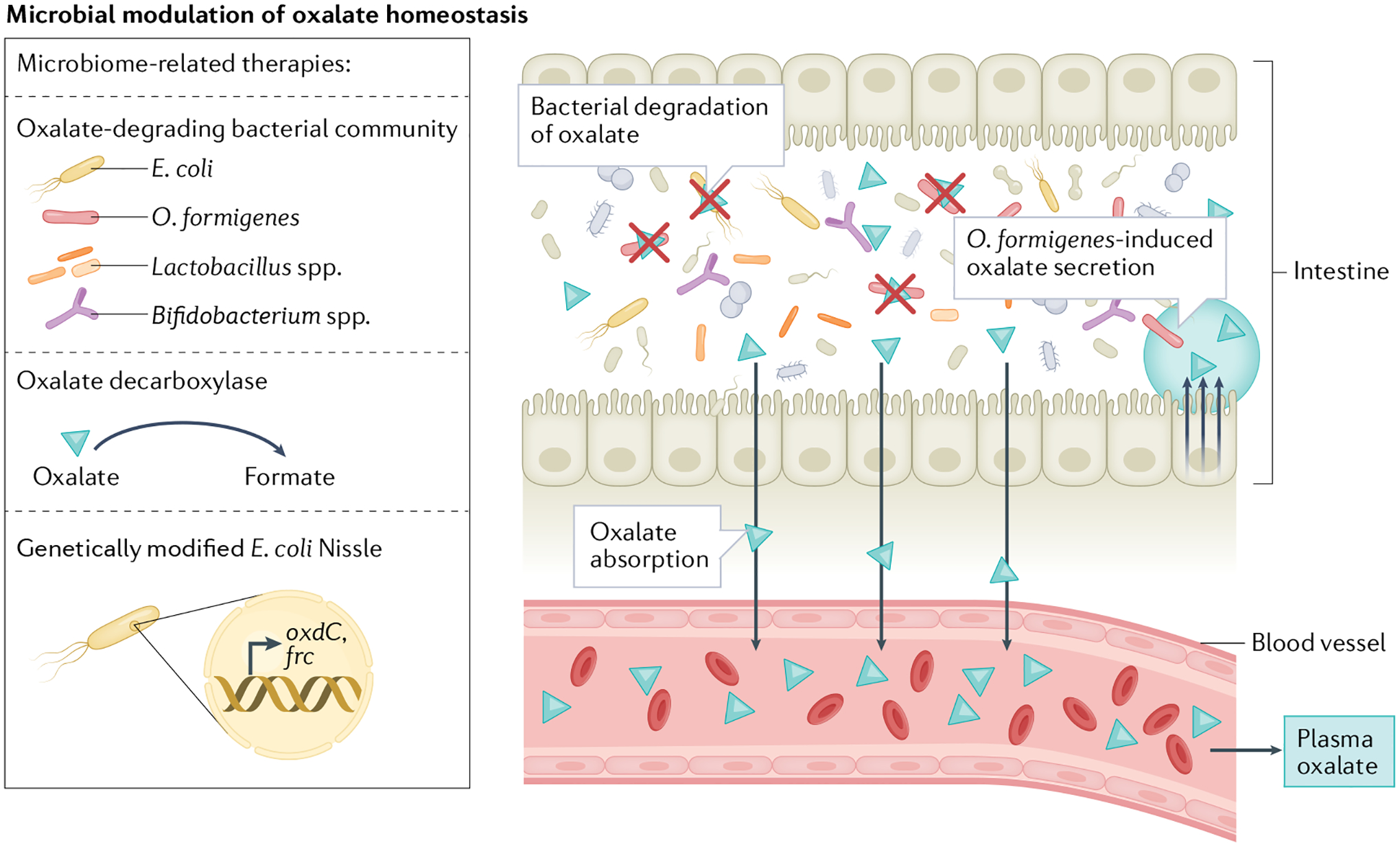
Oxalate homeostasis is maintained through a delicate balance between endogenous sources, exogenous supply and excretion from the body. Novel studies have shed light on the essential roles of metabolic pathways, the microbiome, epithelial oxalate transporters, and adequate oxalate excretion to maintain oxalate homeostasis. In patients with primary or secondary hyperoxaluria, nephrolithiasis, acute or chronic oxalate nephropathy, or chronic kidney disease irrespective of aetiology, one or more of these elements are disrupted. The consequent impairment in oxalate homeostasis can trigger localized and systemic inflammation, progressive kidney disease and cardiovascular complications, including sudden cardiac death. Although kidney replacement therapy is the standard method for controlling elevated plasma oxalate concentrations in patients with kidney failure requiring dialysis, more research is needed to define effective elimination strategies at earlier stages of kidney disease. Beyond well-known interventions (such as dietary modifications), novel therapeutics (such as small interfering RNA gene silencers, recombinant oxalate-degrading enzymes and oxalate-degrading bacterial strains) hold promise to improve the outlook of patients with oxalate-related diseases. In addition, experimental evidence suggests that anti-inflammatory medications might represent another approach to mitigating or resolving oxalate-induced conditions.
© 2022. Springer Nature Limited.
Conflict of interest statement
F.K. reports personal fees from Allena, Oxthera, Sanofi, Fresenius Medical Care, Alnylam Pharmaceuticals, Advicenne, Medice and Zai, and grant support from Alnylam and Dicerna Pharmaceuticals. S.W. reports personal fees from Public Health Advocacy Institute, CVS, Roth Capital Partners, Kantum Pharma, Mallinckrodt, Wolters Kluewer, GE Health Care, GSK, Allena Pharmaceuticals, Mass Medical International, Barron and Budd (versus Fresenius), JNJ, Venbio, Strataca, Takeda, Cerus, Pfizer, Bunch and James, Harvard Clinical Research Institute (also known as Baim Institute for Clinical Research), Oxidien, Sironax, Metro Biotechnology, Biomarin, Bain and Regeneron. L.N. reports personal fees from Oxthera, Dicerna, Federation Bio, Allena, Novome and Synlogic. All other authors declare no competing interests.
Figures
References
-
- Cochat P & Rumsby G Primary hyperoxaluria. N. Engl. J. Med 369, 649–658 (2013). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
