

Brain white matter hyperintensities in Kawasaki disease: A case-control study
- PMID: 36330348
- PMCID: PMC9623056
- DOI: 10.3389/fnins.2022.995480
Brain white matter hyperintensities in Kawasaki disease: A case-control study
Abstract
Background: Cerebrovascular involvement of Kawasaki disease (KD) is poorly studied. White matter hyperintensities (WMH) indicate cerebral small vessel disease and increase the risk for stroke.
Purpose: To investigate whether childhood KD is associated with WMHs and other cerebrovascular findings later in adulthood.
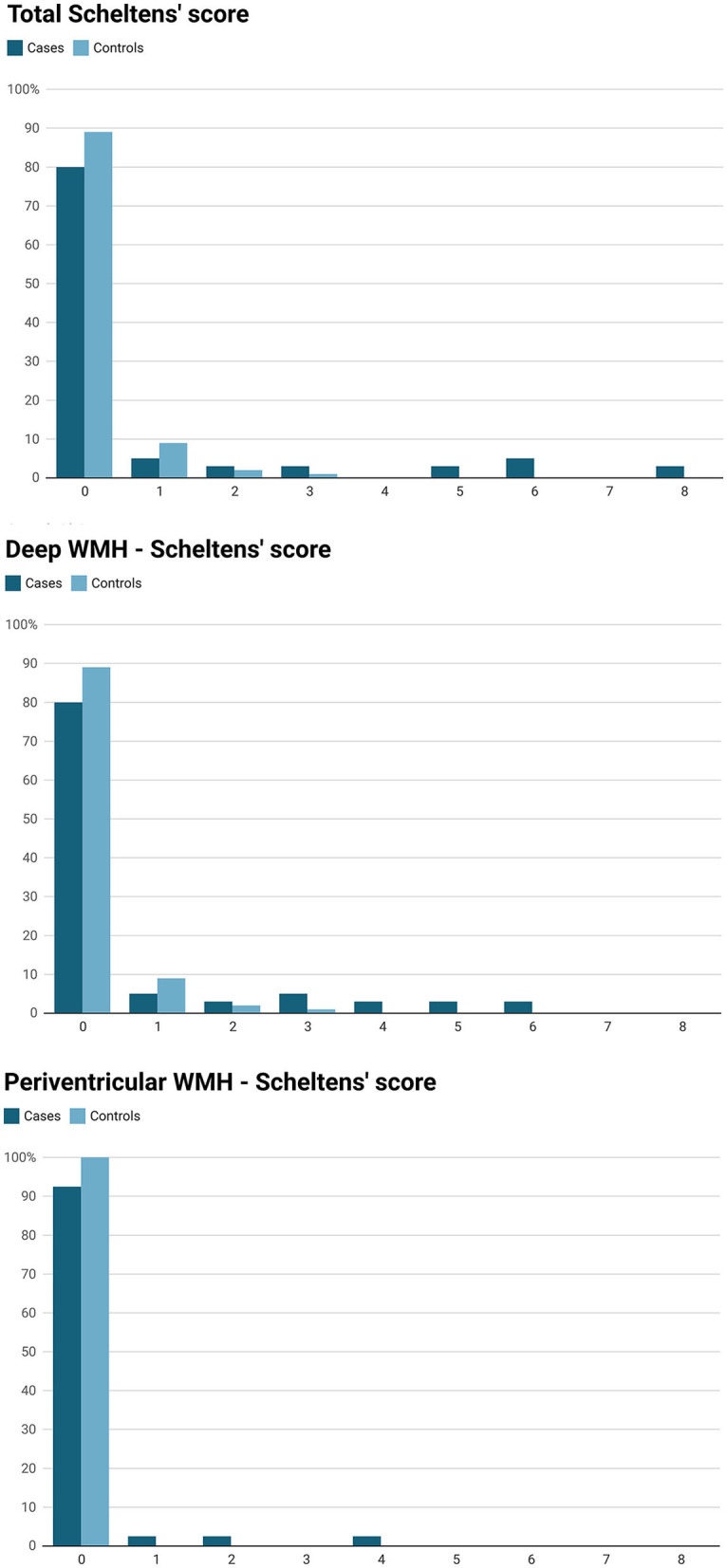
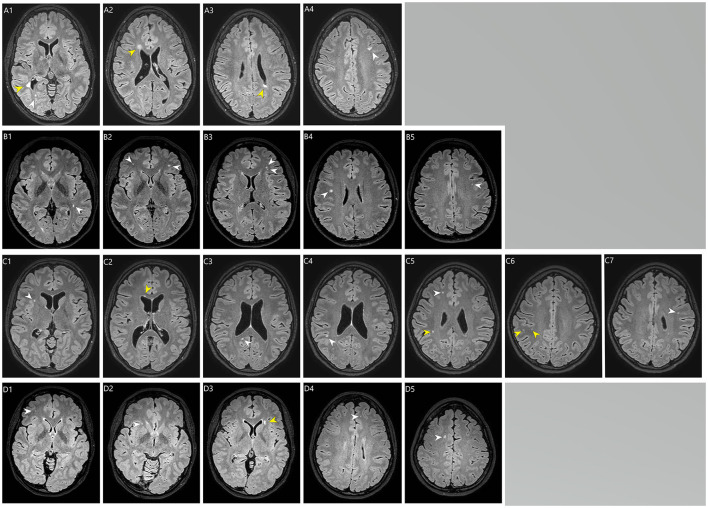
Materials and methods: In this case-control study, patients diagnosed with KD (cases) at our tertiary hospital between 1978 and 1995 were invited to brain magnetic resonance (MRI) between 2016 and 2017. Migraine patients (controls) with available brain MRI were matched with cases (ratio 4:1) by age (±2 years) and sex. Two blinded neuroradiologists evaluated independently cerebrovascular findings from the brain MRI scans. Modified Scheltens' visual rating scale was used to evaluate WMH burden and the total WMH volume was measured using manual segmentation.
Results: Mean age [years, (SD)] at the time of brain MRI was 33.3 (3.8) and 32.8 (4.0) for cases (n = 40) and controls (n = 160), respectively (P = 0.53). Mean follow-up time for cases was 29.5 years (4.3). Total volume of WMHs (median) was 0.26 cm3 (IQR 0.34) for cases and 0.065 cm3 (IQR 0.075) for controls, P = 0.039. Cases had higher total WMH burden (P = 0.003), deep WMH burden (P = 0.003), and more periventricular WMHs (prevalence 7.5 vs. 0%, P = 0.008) than controls. Cases had greater risk of having total Scheltens' score ≥2 vs. < 2 (odds ratio, 6.88; 95% CI: 1.84-25.72, P = 0.0041) and ≥3 vs. < 3 (odds ratio, 22.71; 95% CI: 2.57-200.53, P = 0.0049). Diabetes type 1/type 2, hypertension, smoking status or hypercholesterolemia were not risk factors for WMH burden, p > 0.1. Myocarditis at the acute phase of KD increased the risk for periventricular WMHs (P < 0.05). Three cases (7.5%) and three controls (1.9%) had lacune of presumed vascular origin (P = 0.0096).
Conclusion: History of KD could be associated with an increased WMH burden. More studies are needed to confirm our results.
Keywords: Kawasaki disease; brain MRI; cerebrovascular abnormalities; follow up; white matter hyperintensities.
Copyright © 2022 Laukka, Parkkola, Hirvonen, Ylikotila, Vahlberg, Salo, Kivelev, Rinne and Rahi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Alber J., Alladi S., Bae H. J., Barton D. A., Beckett L. A., Bell J. M., et al. (2019). White matter hyperintensities in vascular contributions to cognitive impairment and dementia (VCID): knowledge gaps and opportunities. Alzheimers Dement. 5, 107–117. 10.1016/j.trci.2019.02.001 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources