

Bispecific antibodies in multiple myeloma treatment: A journey in progress
- PMID: 36330495
- PMCID: PMC9623099
- DOI: 10.3389/fonc.2022.1032775
Bispecific antibodies in multiple myeloma treatment: A journey in progress
Abstract
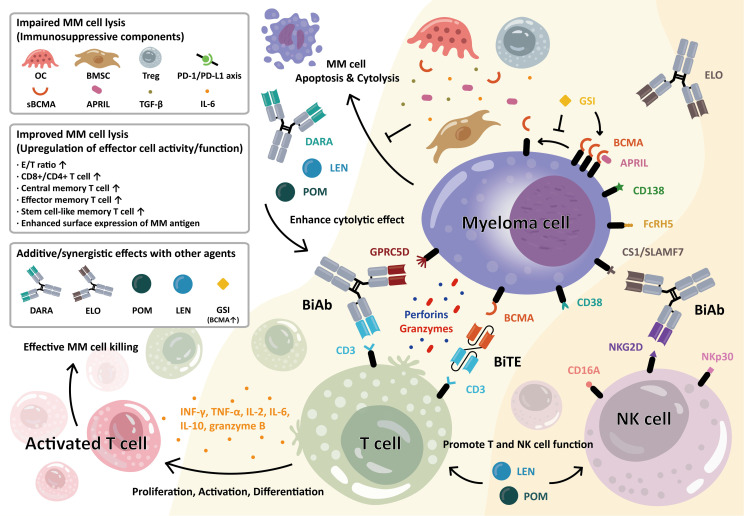
The incorporation of novel agents and monoclonal antibody-based therapies into the treatment of multiple myeloma (MM) has significantly improved long-term patient survival. However, the disease is still largely incurable, with high-risk patients suffering shorter survival times, partly due to weakened immune systems. Bispecific molecules, including bispecific antibodies (BisAbs) and bispecific T-cell engagers (BiTEs), encourage immune cells to lyse MM cells by simultaneously binding antigens on MM cells and immune effector cells, bringing those cells into close proximity. BisAbs that target B-cell maturation antigen (BCMA) and GPRC5D have shown impressive clinical activity, and the results of early-phase clinical trials targeting FcRH5 in patients with relapsed/refractory MM (RRMM) are also promising. Furthermore, the safety profile of these agents is favorable, including mainly low-grade cytokine release syndrome (CRS). These off-the-shelf bispecific molecules will likely become an essential part of the MM treatment paradigm. Here, we summarize and highlight various bispecific immunotherapies under development in MM treatment, as well as the utility of combining them with current standard-of-care treatments and new strategies. With the advancement of novel combination treatment approaches, these bispecific molecules may lead the way to a cure for MM.
Keywords: BCMA; CD38; FcRH5; GPRC5D; bispecific T-cell engager; bispecific antibody; immunotherapy; multiple myeloma.
Copyright © 2022 Cho, Yeh, Anderson and Tai.
Conflict of interest statement
Author KA serves on advisory boards to Pfizer, Amgen, AstraZeneca, Janssen, Precision Biosciences, Window, and Starton, and is a scientific founder of OncoPep, C4 Therapeutics, Raqia, and NextRNA. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Durie BGM, Hoering A, Abidi MH, Rajkumar SV, Epstein J, Kahanic SP, et al. . Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): A randomised, open-label, phase 3 trial. Lancet (2017) 389(10068):519–27. doi: 10.1016/S0140-6736(16)31594-X - DOI - PMC - PubMed
-
- Rosinol L, Oriol A, Teruel AI, Hernandez D, Lopez-Jimenez J, de la Rubia J, et al. . Superiority of bortezomib, thalidomide, and dexamethasone (VTD) as induction pretransplantation therapy in multiple myeloma: A randomized phase 3 PETHEMA/GEM study. Blood (2012) 120(8):1589–96. doi: 10.1182/blood-2012-02-408922 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials