

Preterm Brain Injury and Neurodevelopmental Outcomes: A Meta-analysis
- PMID: 36330752
- PMCID: PMC9724175
- DOI: 10.1542/peds.2022-057442
Preterm Brain Injury and Neurodevelopmental Outcomes: A Meta-analysis
Abstract
Context: Preterm brain injuries are common; neurodevelopmental outcomes following contemporary neonatal care are continually evolving.
Objective: To systematically review and meta-analyze neurodevelopmental outcomes among preterm infants after intraventricular hemorrhage (IVH) and white matter injury (WMI).
Data sources: Published and grey literature were searched across 10 databases between 2000 and 2021.
Study selection: Observational studies reporting 3-year neurodevelopmental outcomes for preterm infants with IVH or WMI compared with preterm infants without injury.
Data extraction: Study characteristics, population characteristics, and outcome data were extracted.
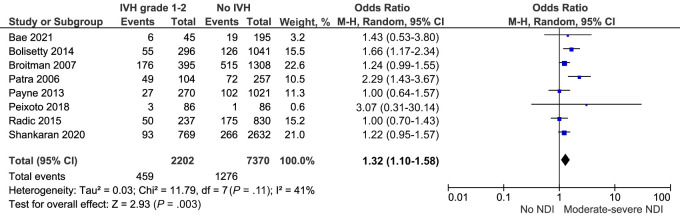
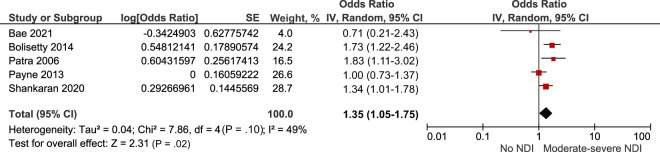
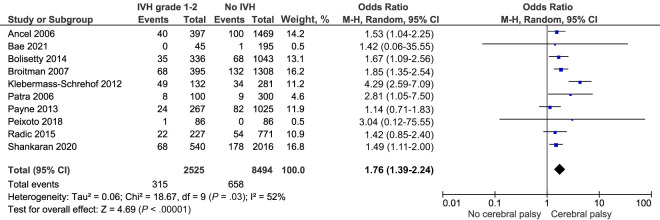
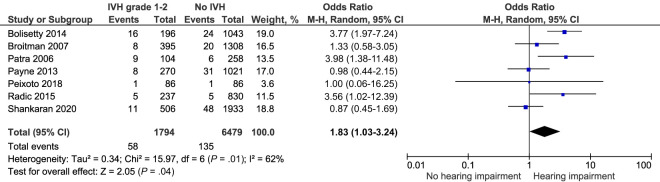
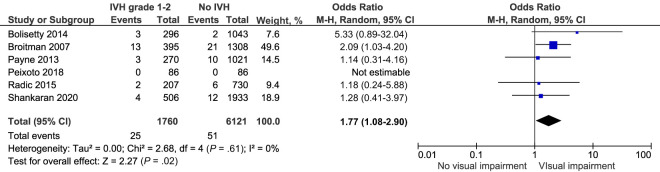
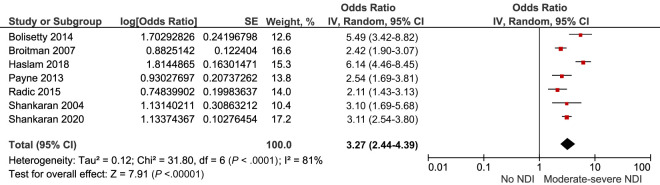
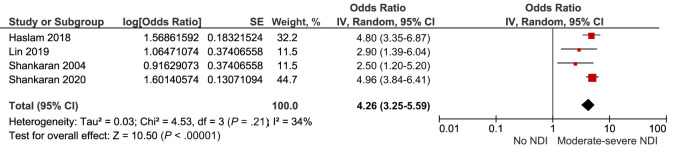
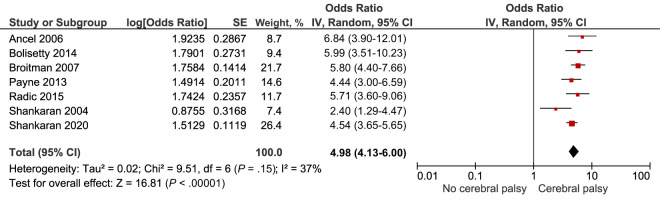
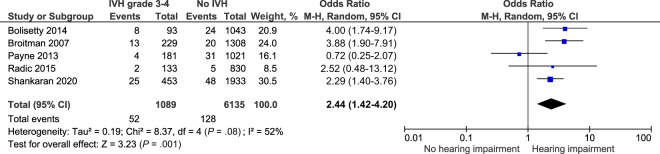
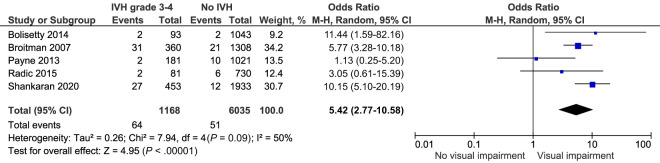
Results: Thirty eight studies were included. There was an increased adjusted risk of moderate-severe neurodevelopmental impairment after IVH grade 1 to 2 (adjusted odds ratio 1.35 [95% confidence interval 1.05-1.75]) and IVH grade 3 to 4 (adjusted odds ratio 4.26 [3.25-5.59]). Children with IVH grade 1 to 2 had higher risks of cerebral palsy (odds ratio [OR] 1.76 [1.39-2.24]), cognitive (OR 1.79 [1.09-2.95]), hearing (OR 1.83 [1.03-3.24]), and visual impairment (OR 1.77 [1.08-2.9]). Children with IVH grade 3 to 4 had markedly higher risks of cerebral palsy (OR 4.98 [4.13-6.00]), motor (OR 2.7 [1.52-4.8]), cognitive (OR 2.3 [1.67-3.15]), hearing (OR 2.44 [1.42-4.2]), and visual impairment (OR 5.42 [2.77-10.58]). Children with WMI had much higher risks of cerebral palsy (OR 14.91 [7.3-30.46]), motor (OR 5.3 [3-9.36]), and cognitive impairment (OR 3.48 [2.18-5.53]).
Limitations: Heterogeneity of outcome data.
Conclusions: Mild IVH, severe IVH, and WMI are associated with adverse neurodevelopmental outcomes. Utilization of core outcome sets and availability of open-access study data would improve our understanding of the nuances of these outcomes.
Conflict of interest statement
Figures

References
-
- Harrison MS, Goldenberg RL. Global burden of prematurity. Semin Fetal Neonatal Med. 2016;21(2):74–79 - PubMed
-
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172 - PubMed
