

Time to decision in sepsis
- PMID: 36331185
- PMCID: PMC9910674
- DOI: 10.37201/req/083.2022
Time to decision in sepsis
Abstract
Objective: This study aimed to identify the common barriers leading to delayed initial management, microbiological diagnosis, and appropriate empirical antimicrobial treatment in sepsis.
Methods: A cross-sectional study was performed by the application of a population-based survey. Four different surveys were designed, targeting the healthcare personnel located in main hospital areas [emergency department (SEMES); infectious diseases and clinical microbiology-microbiological diagnosis (SEIMC-M); intensive care and infectious diseases, (SEMICYUC-GTEIS); and infectious diseases and clinical microbiology-clinical diagnosis, (SEIMC-C)].
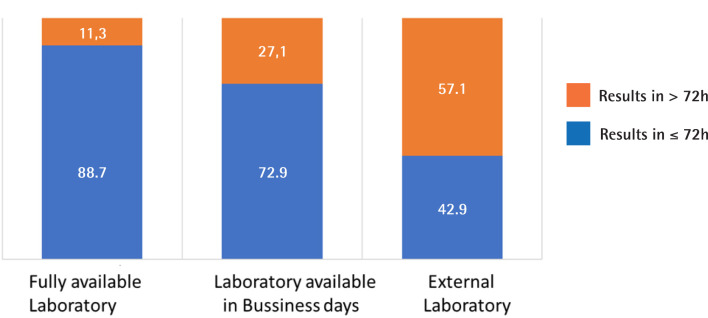
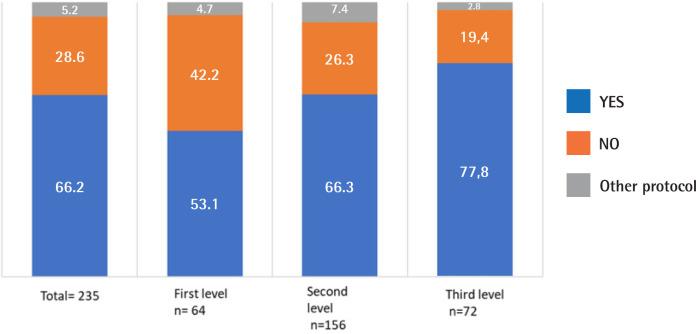
Results: A total of 700 valid surveys were collected from June to November 2019: 380 (54.3%) of SEMES, 127 (18.1%) of SEIMC-M, 97 (13.9%) de SEMICYUC-GTEIS and 96 (13.7%) of SEIMC-C, in 270 hospitals of all levels of care. The qSOFA score was used as a screening tool. The most used biomarker was procalcitonin (n=92, 39.8%). The sepsis code was implemented in 157 of 235 participating centers (66.2%), particularly in tertiary level hospitals. The mean frequency of contaminated blood cultures was 8.9% (8.7). In 85 (78.7%) centers, positive results of blood cultures were available within the first 72 hours and were communicated to the treating physician effectively by phone or e-mail in 76 (81.7%) cases. The main reason for escalating treatment was clinical deterioration, and the reason for de-escalating antimicrobials was significantly different between the specialties. Quality indicators were not frequently monitored among the different participating centers.
Conclusions: There are significant barriers that hinder adequate management processes in sepsis in Spanish hospitals.
Introducción: Este estudio tuvo como objetivo identificar las barreras comunes que conducen al retraso en el manejo inicial, el diagnóstico microbiológico y el tratamiento antimicrobiano empírico adecuado en la sepsis.
Pacientes y métodos: Se realizó un estudio transversal mediante la aplicación de una encuesta de base poblacional. Se diseñaron cuatro encuestas diferentes, dirigidas al personal de salud ubicado en las principales áreas hospitalarias [urgencias (SEMES); enfermedades infecciosas y microbiología clínica-diagnóstico microbiológico (SEIMC-M); cuidados intensivos y enfermedades infecciosas (SEMICYUC-GTEIS); y enfermedades infecciosas y microbiología clínica-diagnóstico clínico, (SEIMC-C)].
Resultados: Se recogieron un total de 700 encuestas válidas de junio a noviembre de 2019: 380 (54,3%) de SEMES, 127 (18,1%) de SEIMC-M, 97 (13,9%) de SEMICYUC-GTEIS y 96 (13,7%) de la SEIMC-C, en 270 hospitales de todos los niveles de atención. El qSOFA se utilizó principalmente como herramienta de detección. El biomarcador más utilizado fue la procalcitonina (n=92, 39,8%). El código sepsis estaba implementado en 157 de 235 centros participantes (66,2%), particularmente en hospitales de tercer nivel. La frecuencia media de hemocultivos contaminados fue del 8,9% (8,7). En 85 (78,7%) de los centros, los resultados de los hemocultivos positivos estuvieron disponibles en las primeras 72 horas y se comunicaron al médico responsable del paciente por teléfono o correo electrónico en 76 casos (81,7%). El motivo principal de la escalada del tratamiento fue el deterioro clínico y el motivo de la desescalada de los antimicrobianos fue significativamente diferente entre las especialidades. Los indicadores de calidad no se monitorizaban con frecuencia en los diferentes centros.
Conclusión: Existen importantes barreras que dificultan los procesos de manejo adecuado de la sepsis en los hospitales españoles.
Keywords: Sepsis Code; Sepsis management; quality indicators.
©The Author 2022. Published by Sociedad Española de Quimioterapia. This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)(https://creativecommons.org/licenses/by-nc/4.0/).
Conflict of interest statement
MNL has participated as a speaker at scientific meetings sponsored by Accelerate Diagnostics and bioMérieux.
Figures
References
-
- Rüddel H, Thomas-Rüddel DO, Reinhart K, Bach F, Gerlach H, Lind-ner M, et al. . Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial. Crit Care. 2022;26(1):51. DOI: 10.1186/s13054-022-03901-9 - DOI - PMC - PubMed
-
- Simmonds M, Hutchinson A, Chikhani M, Bewick T, Meyer J, Davies SR, et al. . Surviving Sepsis beyond Intensive Care: A Retrospective Cohort Study of Compliance with the International Guidelines. Journal of the Intensive Care Society. 2008;9:124-7.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
