

Inclisiran and cardiovascular events: a patient-level analysis of phase III trials
- PMID: 36331326
- PMCID: PMC9825807
- DOI: 10.1093/eurheartj/ehac594
Inclisiran and cardiovascular events: a patient-level analysis of phase III trials
Abstract
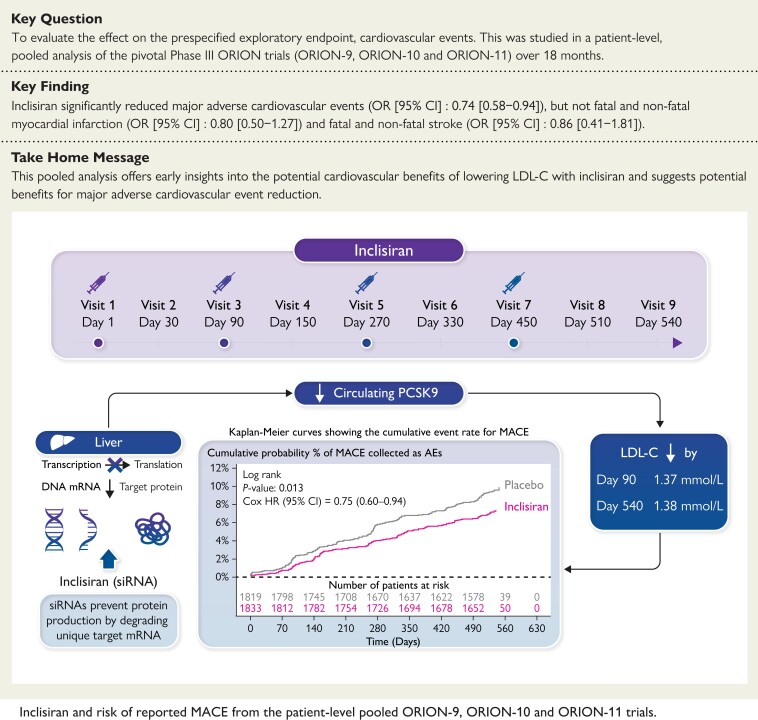
Background: Inclisiran, an siRNA administered twice-yearly, significantly reduced LDL cholesterol (LDL-C) in Phase III trials. Whether lowering LDL-C with inclisiran translates into a lower risk of cardiovascular (CV) events is not yet established.
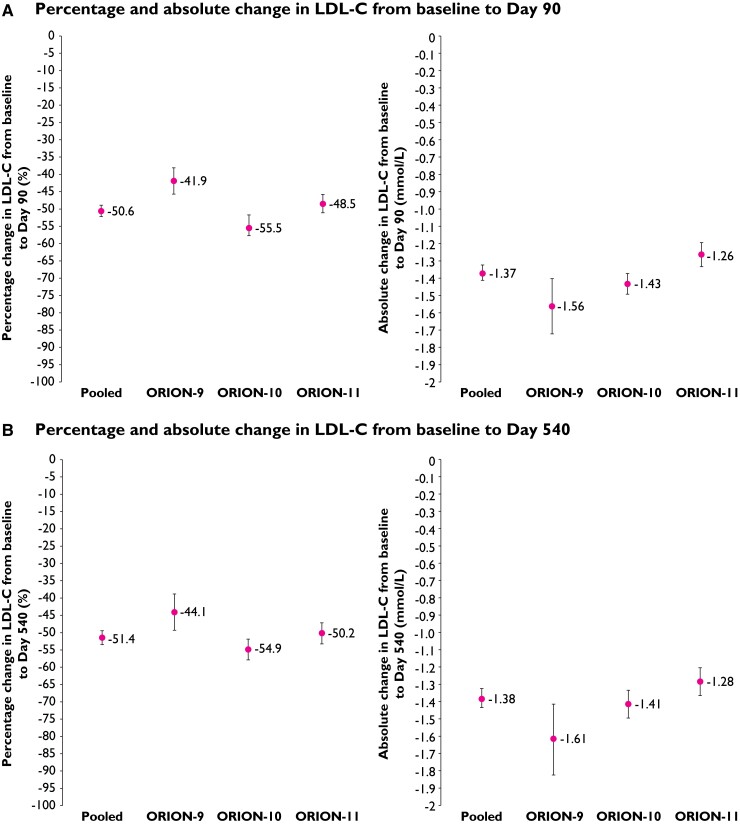
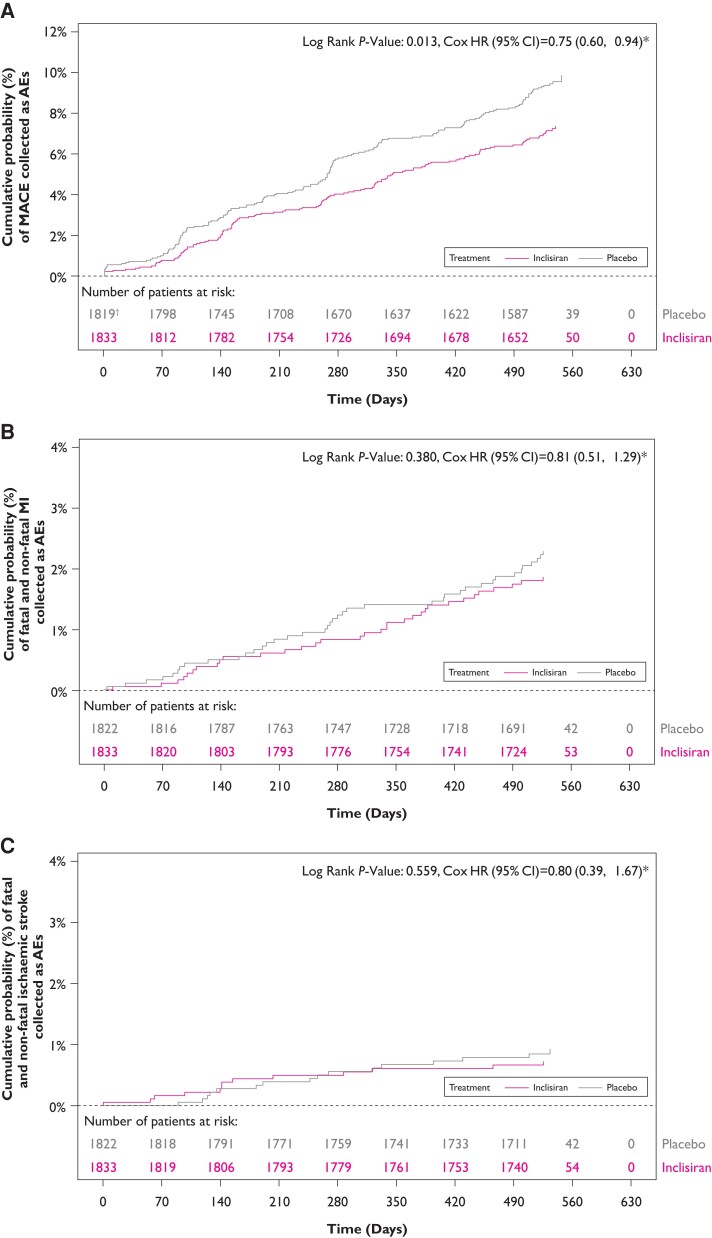
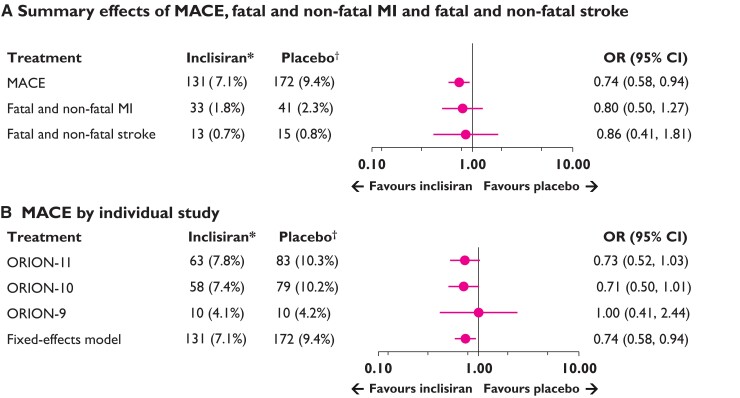
Methods and results: Patient-level, pooled analysis of ORION-9, -10 and -11, included patients with heterozygous familial hypercholesterolaemia, atherosclerotic CV disease (ASCVD), or ASCVD risk equivalent on maximally tolerated statin-therapy, randomized 1:1 to receive 284 mg inclisiran or placebo on Days 1, 90, and 6-monthly thereafter for 18 months. Prespecified exploratory endpoint of major cardiovascular events (MACEs) included non-adjudicated CV death, cardiac arrest, non-fatal myocardial infarction (MI), and fatal and non-fatal stroke, evaluated as part of safety assessments using a standard Medical Dictionary for Regulatory Activities basket. Although not prespecified, total fatal and non-fatal MI, and stroke were also evaluated. Mean LDL-C at baseline was 2.88 mmol/L. At Day 90, the placebo-corrected percentage reduction in LDL-C with inclisiran was 50.6%, corresponding to an absolute reduction of 1.37 mmol/L (both P < 0.0001). Among 3655 patients over 18 months, 303 (8.3%) experienced MACE, including 74 (2.0%) fatal and non-fatal MIs, and 28 (0.8%) fatal and non-fatal strokes. Inclisiran significantly reduced composite MACE [OR (95% CI): 0.74 (0.58-0.94)], but not fatal and non-fatal MIs [OR (95% CI): 0.80 (0.50-1.27)] or fatal and non-fatal stroke [OR (95% CI): 0.86 (0.41-1.81)].
Conclusion: This analysis offers early insights into the potential CV benefits of lowering LDL-C with inclisiran and suggests potential benefits for MACE reduction. These findings await confirmation in the larger CV outcomes trials of longer duration.
Keywords: Atherosclerotic cardiovascular disease; Inclisiran; LDL-C; Major adverse cardiovascular events.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: K.K.R. receives support from the National Institute for Health Research (NIHR) Imperial Biomedical Research Centre; his institution (Imperial College London) receives support from the NIHR Applied Research Collaboration Northwest London. K.K.R. reports receiving lecture fees from Aegerion Pharmaceuticals, Kowa, Cipla, Algorithm, and Zuelling Pharma, grant support, paid to his institution, lecture fees, and advisory board fees from Amgen, Regeneron Pharmaceuticals/Sanofi, and Pfizer, lecture fees and fees for serving on steering committees for trials from AstraZeneca and Eli Lilly, fees for serving on steering committees for trials from Cerenis Therapeutics, The Medicines Company, and Esperion, advisory board fees from Akcea Therapeutics, Novartis, Silence Therapeutics, Bayer, and Daiichi Sankyo, lecture fees and advisory board fees from Takeda, Boehringer Ingelheim, and Dr Reddy’s Laboratories, grant support and advisory board fees from Merck Sharp & Dohme, fees for serving on a clinical events adjudication committee from AbbVie, and fees for serving as principal investigator for a trial from Resverlogix. F.J.R. reports receiving advisory board fees and lecture fees from Amgen, Sanofi-Aventis, Regeneron Pharmaceuticals, The Medicines Company and Novartis. D.G.K. reports being employed by and holding stock options in the Medicines Company at the time of study and employment with DalCor Pharmaceuticals and LIB Therapeutics at the time of publication. M.J.J. has received fees for providing statistical analysis for trials from The Medicines Company and Novartis. W.K. reports receiving consulting fees and lecture fees from AstraZeneca, Novartis and Amgen, consulting fees from Pfizer, the Medicines Company and Novartis, DalCor Pharmaceuticals, Kowa, Corvidia Therapeutics, Esperion, Genentech, OMEICOS, Novo Nordisk, LIB Therapeutics, and Daiichi Sankyo, lecture fees from Berlin-Chemie, Bristol-Myers Squibb and Sanofi, and grant support and provision of reagents from Singulex, Abbott, Roche Diagnostics, and Dr Beckmann Pharma. L.A.L. grant support paid to his institution, advisory board fees and fees for CME from Amgen, and Novartis; fees for serving on a steering committee and advisory board fees from Esperion; grant support paid to his institution and fees for serving on a steering committee from Kowa, and the Medicines Company and Novartis; advisory board fees and fees for CME from Amarin, Astra Zeneca, HLS, Merck, Pfizer, and Sanofi. U.L. reports receiving lecture and/or advisory fees from AstraZeneca, Boehringer, Sanofi, Berlin Chemie, and Abbott, advisory fees from The Medicines Company, and grant support to institution, lecture fees, and advisory fees from Amgen, Bayer and Novartis. G.G.S. reports receiving research support, paid to his institution, from AstraZeneca, Resverlogix, Sanofi, Silence Therapeutics, and The Medicines Company, and a patent (62/806313) on a method for reducing cardiovascular risk assigned in full to the University of Colorado. D.L. reports being employed by Novartis at the time of publication and holding shares in Novartis. A.F. reports being employed by and holding shares and stock options in The Medicines Company at the time of the clinical study and was employed by Novartis at the time of analysis. L.G.C. reports being employed by Novartis at the time of publication. R.S.W. reports receiving advisory board fees from Boehringer Ingelheim and past fees for consulting on lipid issues with the Medicines Company.
Figures
Comment in
-
Cholesterol lowering with inclisiran: a new chapter in the PCSK9 story book.Eur Heart J. 2023 Jan 7;44(2):139-141. doi: 10.1093/eurheartj/ehac656. Eur Heart J. 2023. PMID: 36331316 No abstract available.
References
-
- Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. . Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J 2017;38:2459–2472. 10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
