

Short-term efficacy of angiotensin receptor-neprilysin inhibitor treatment in patients with ST-segment elevation myocardial infarction with reduced ejection fraction after primary percutaneous coronary intervention: a propensity score matching study
- PMID: 36333668
- PMCID: PMC9636690
- DOI: 10.1186/s12872-022-02906-0
Short-term efficacy of angiotensin receptor-neprilysin inhibitor treatment in patients with ST-segment elevation myocardial infarction with reduced ejection fraction after primary percutaneous coronary intervention: a propensity score matching study
Abstract
Background: Acute myocardial infarction (AMI) causes a series of pathophysiological changes, including myocardial necrosis, myocardial edema, and microvascular damage. These changes eventually lead to severe cardiovascular events, such as ventricular remodeling, heart failure, and papillary dysfunction. Impaired cardiac function after ST-segment elevation myocardial infarction (STEMI) often manifests as a decrease in left ventricular ejection fraction (LVEF). Clinical trials have shown that angiotensin receptor-neprilysin inhibitor (ARNI) treatment has the potential to improve LVEF in patients with STEMI after primary percutaneous coronary intervention (PPCI).
Objective: The purpose of this study was to evaluate the short-term efficacy of ARNI versus angiotensin-converting enzyme inhibitor (ACEI) treatment in patients with STEMI who exhibit reduced LVEF after PPCI.
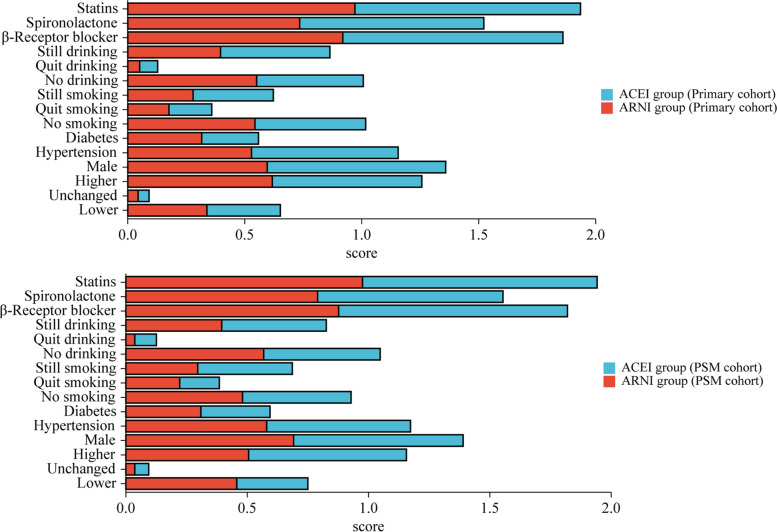
Methods: A total of 169 patients with STEMI exhibiting post-PPCI LVEF below 50% who were orally treated with ARNI between December 2017 and August 2020 were selected as the experimental group. A total of 136 patients with STEMI exhibiting post-PPCI LVEF below 50% who were orally treated with an ACEI between January 2016 and August 2020 were selected as the control group. LVEF was measured using cardiac ultrasonography during hospitalization and 3 months after discharge. Linear and logistic regression analyses were performed to compare patient demographics and hospitalization variables to evaluate the risk factors for change and rate of improvement in LVEF. Propensity score matching (PSM) was used to account for confounding factors.
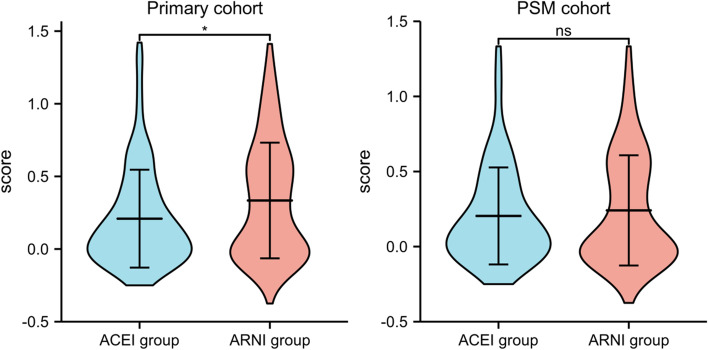
Results: After PSM, the study cohort consisted of 81 patients in the ARNI group and 123 in the ACEI group. After an average follow-up period of 3 months, no significant difference was noted in the LVEF improvement rate between the experimental and control groups (P = 0.475, 95% CI: -0.062 to 0.134). Multivariate logistic regression analysis also indicated no significant correlation between the change in LVEF and oral ARNI treatment in patients with STEMI exhibiting reduced LVEF after PPCI (P > 0.05).
Conclusion: The short-term effect of ARNI treatment on the cardiac function of patients with STEMI and reduced LVEF after PPCI is not superior to that of ACEI treatment.
Keywords: Angiotensin receptor-neprilysin inhibitor; Angiotensin-converting enzyme inhibitor; Primary percutaneous coronary intervention; ST-segment elevation myocardial infarction; Ventricular remodeling.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
