

Social and Psychosocial Determinants of Racial and Ethnic Differences in Cardiovascular Health in the United States Population
- PMID: 36334260
- PMCID: PMC9852071
- DOI: 10.1161/CIRCULATIONAHA.122.061991
Social and Psychosocial Determinants of Racial and Ethnic Differences in Cardiovascular Health in the United States Population
Abstract
Background: Social and psychosocial factors are associated with cardiovascular health (CVH). Our objective was to examine the contributions of individual-level social and psychosocial factors to racial and ethnic differences in population CVH in the NHANES (National Health and Nutrition Examination Surveys) 2011 to 2018, to inform strategies to mitigate CVH inequities.
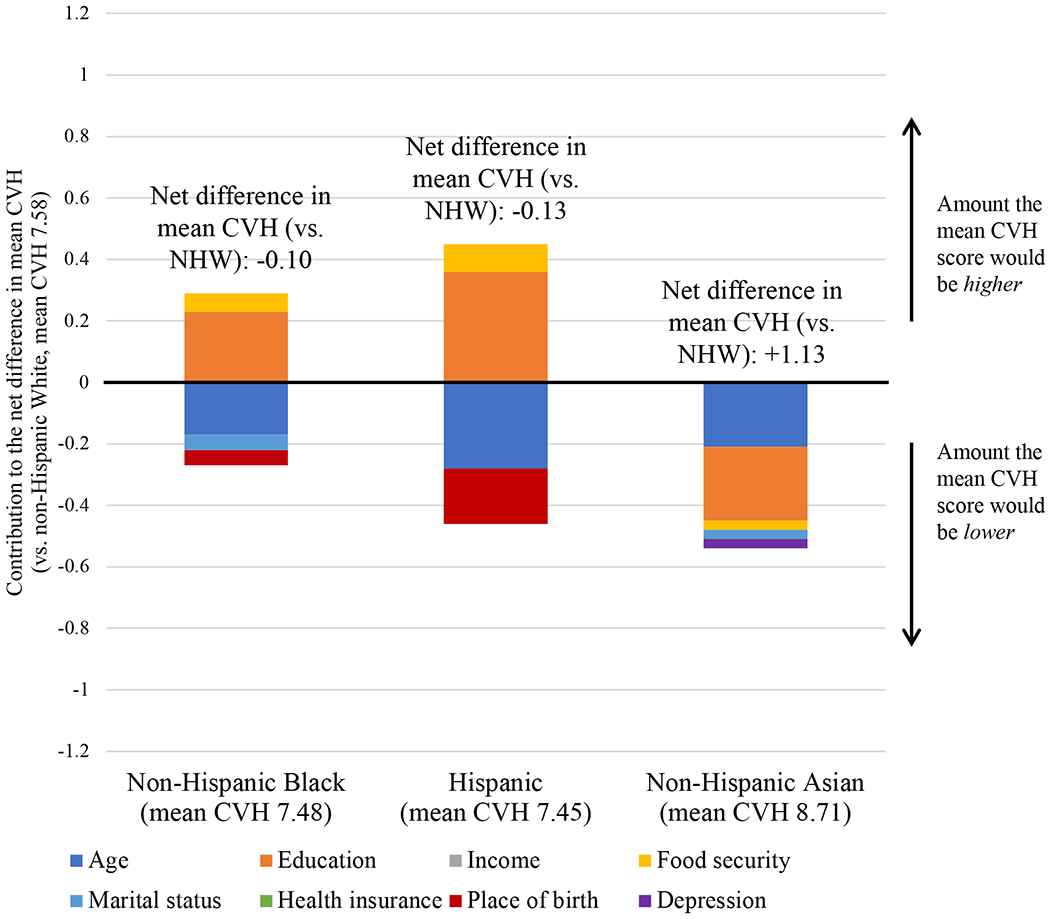
Methods: In NHANES participants ages ≥20 years, Kitagawa-Blinder-Oaxaca decomposition estimated the statistical contribution of individual-level factors (education, income, food security, marital status, health insurance, place of birth, depression) to racial and ethnic differences in population mean CVH score (range, 0-14, accounting for diet, smoking, physical activity, body mass index, blood pressure, cholesterol, blood glucose) among Hispanic, non-Hispanic Asian, or non-Hispanic Black adults compared with non-Hispanic White adults.
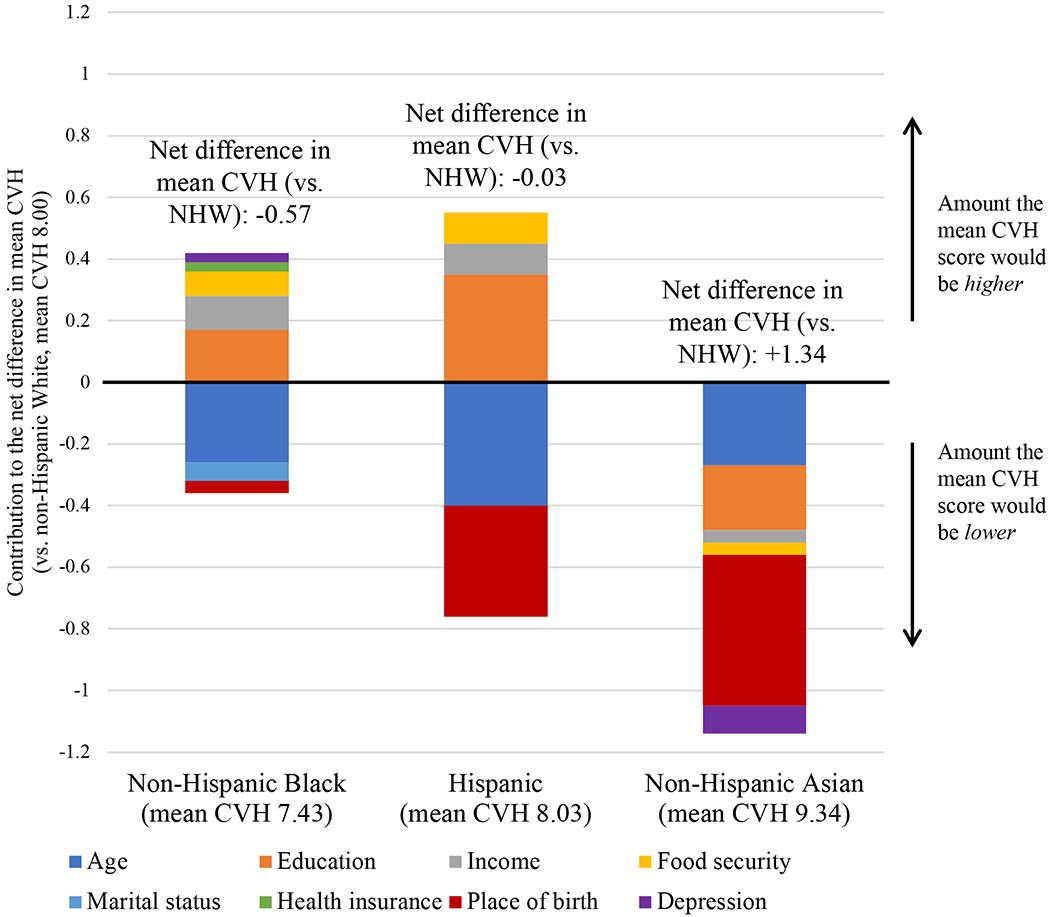
Results: Among 16 172 participants (representing 255 million US adults), 24% were Hispanic, 12% non-Hispanic Asian, 23% non-Hispanic Black, and 41% non-Hispanic White. Among men, mean (SE) CVH score was 7.45 (2.3) in Hispanic, 8.71 (2.2) in non-Hispanic Asian, 7.48 (2.4) in non-Hispanic Black, and 7.58 (2.3) in non-Hispanic White adults. In Kitagawa-Blinder-Oaxaca decomposition, education explained the largest component of CVH differences among men (if distribution of education were similar to non-Hispanic White participants, CVH score would be 0.36 [0.04] points higher in Hispanic, 0.24 [0.04] points lower in non-Hispanic Asian, and 0.23 [0.03] points higher in non-Hispanic Black participants; P<0.05). Among women, mean (SE) CVH score was 8.03 (2.4) in Hispanic, 9.34 (2.1) in non-Hispanic Asian, 7.43 (2.3) in non-Hispanic Black, and 8.00 (2.5) in non-Hispanic White adults. Education explained the largest component of CVH difference in non-Hispanic Black women (if distribution of education were similar to non-Hispanic White participants, CVH score would be 0.17 [0.03] points higher in non-Hispanic Black participants; P<0.05). Place of birth (born in the United States versus born outside the United States) explained the largest component of CVH difference in Hispanic and non-Hispanic Asian women (if distribution of place of birth were similar to non-Hispanic White participants, CVH score would be 0.36 [0.07] points lower and 0.49 [0.16] points lower, respectively; P<0.05).
Conclusions: Education and place of birth confer the largest statistical contributions to the racial and ethnic differences in mean CVH score among US adults.
Keywords: cardiovascular health; ethnicity; psychosocial factors; racial groups; social factors.
Conflict of interest statement
Conflict of Interest Disclosures
The authors report no disclosures or conflicts of interest.
Figures
References
-
- Shah NS, Ning H, Petito LC, Kershaw KN, Bancks MP, Reis JP, Rana JS, Sidney S, Jacobs DR Jr., Kiefe CI, Carnethon MR, Lloyd-Jones DM, Allen NB and Khan SS. Associations of Clinical and Social Risk Factors With Racial Differences in Premature Cardiovascular Disease. Circulation. 2022:101161CIRCULATIONAHA121058311. - PMC - PubMed
-
- Havranek EP, Mujahid MS, Barr DA, Blair IV, Cohen MS, Cruz-Flores S, Davey-Smith G, Dennison-Himmelfarb CR, Lauer MS, Lockwood DW, Rosal M and Yancy CW. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2015;132:873–98. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
