

Comprehensive clinicopathological and genomic profiling of gallbladder cancer reveals actionable targets in half of patients
- PMID: 36335173
- PMCID: PMC9637208
- DOI: 10.1038/s41698-022-00327-y
Comprehensive clinicopathological and genomic profiling of gallbladder cancer reveals actionable targets in half of patients
Abstract
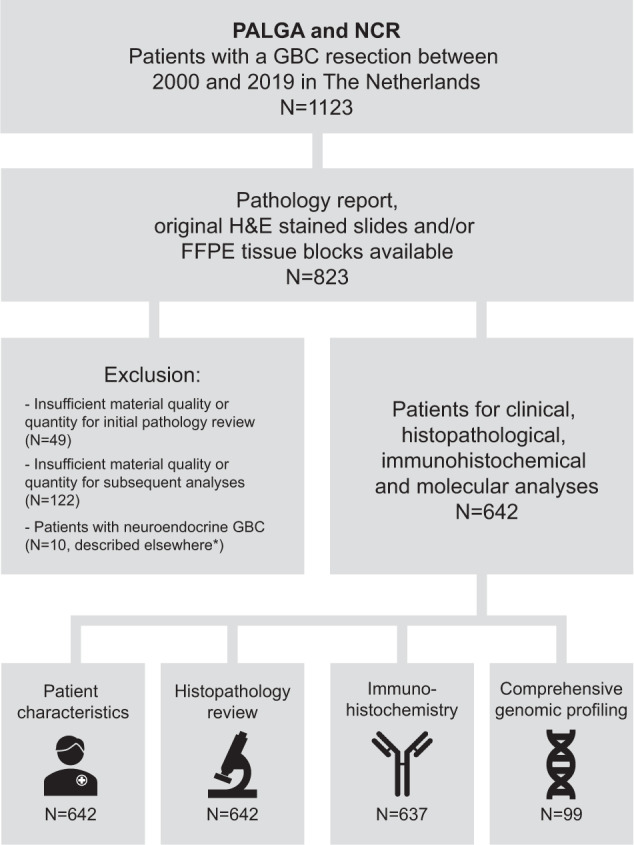
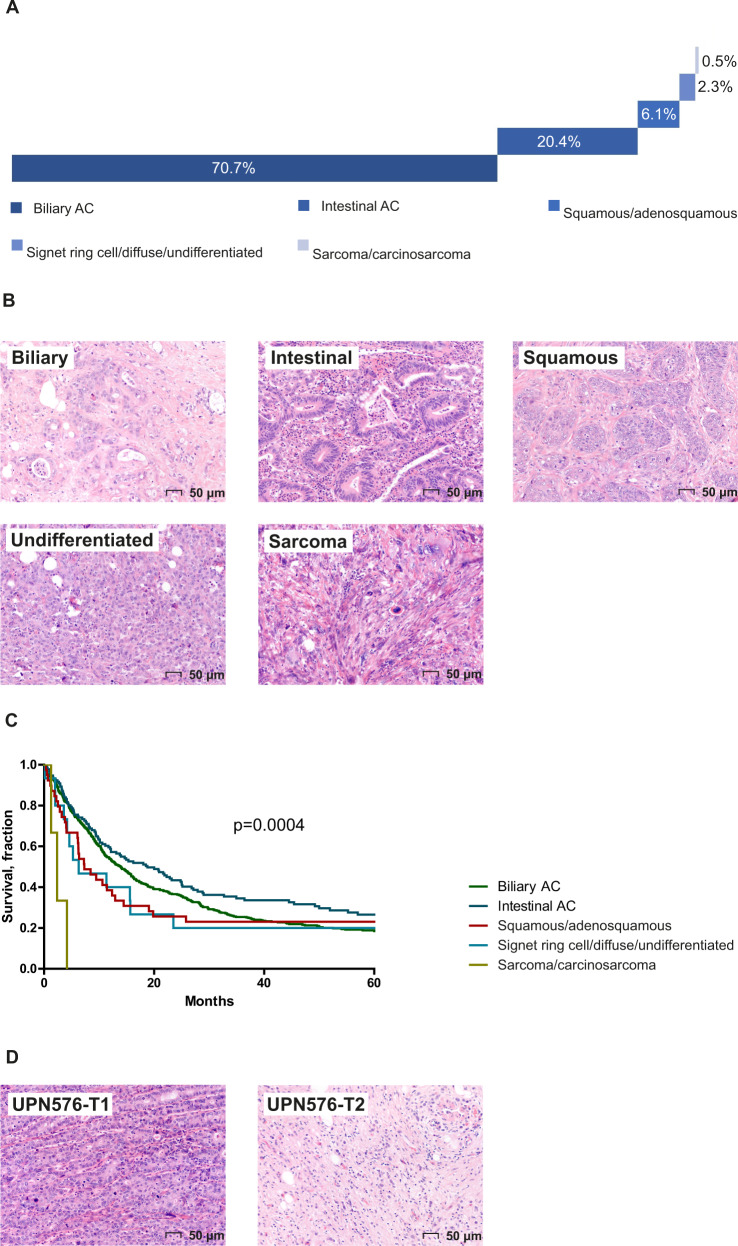
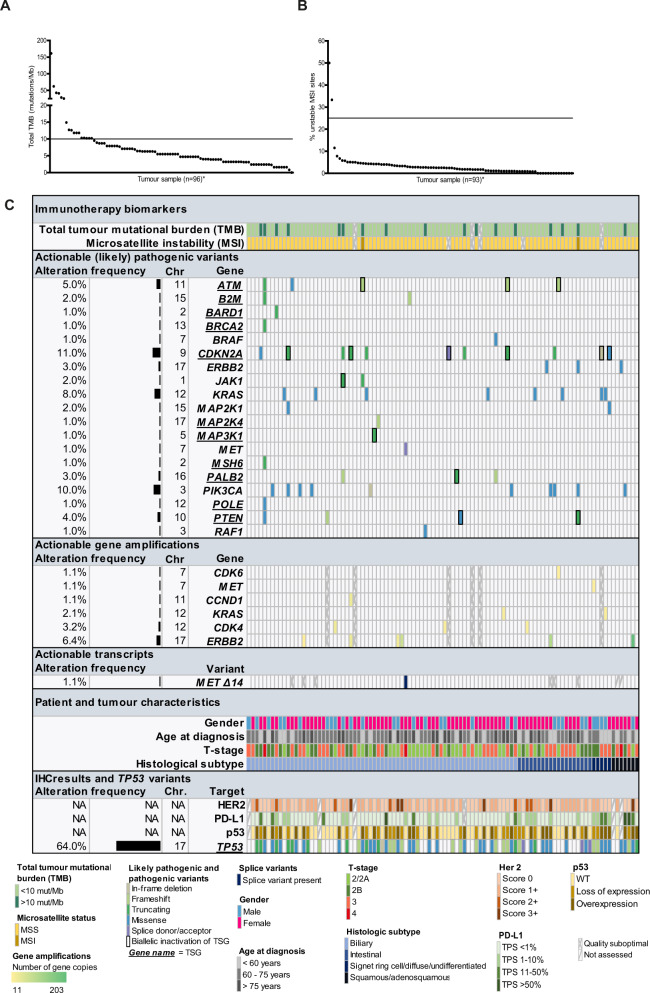
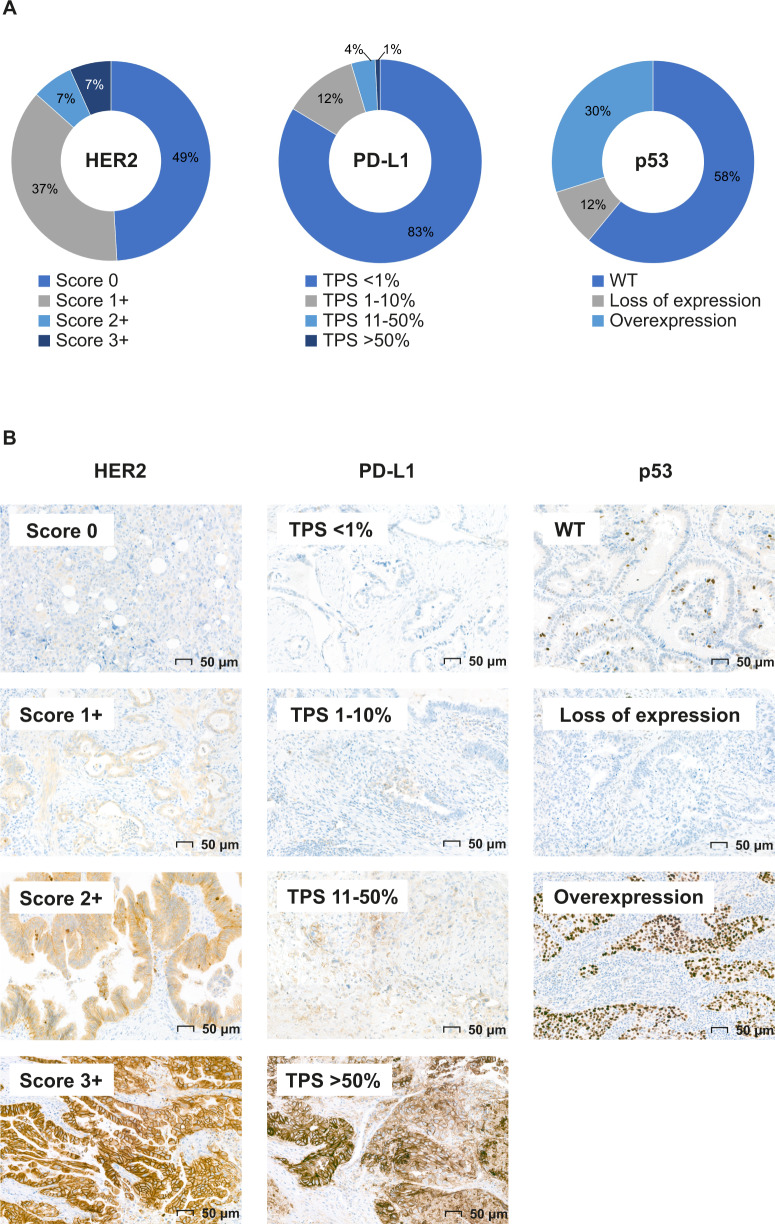
Gallbladder cancer (GBC) is a rare, highly aggressive malignancy with a 5-year survival rate of 5-10% in advanced cases, highlighting the need for more effective therapies. The aim of this study was to identify potentially actionable therapeutic targets for GBC. Specimens and clinicopathological data of 642 GBC patients, diagnosed between 2000 and 2019 were collected using the Dutch Pathology Registry (PALGA) and the Netherlands Cancer Registry. All cases were histologically reviewed and a subset was subjected to a comprehensive next generation sequencing panel. We assessed mutations and gene amplifications in a panel of 54 actionable genes, tumor-mutational burden (TMB), and microsatellite instability (MSI). Additionally, the entire cohort was screened for HER2, PD-L1, pan-TRK, and p53 expression with immunohistochemistry. Histopathological subtypes comprised biliary-type adenocarcinoma (AC, 69.6%), intestinal-type AC (20.1%) and other subtypes (10.3%). The median total TMB was 5.5 mutations/Mb (range: 0-161.1) and 17.7% of evaluable cases had a TMB of >10 mutations/Mb. MSI was observed in two cases. Apart from mutations in TP53 (64%), tumors were molecularly highly heterogeneous. Half of the tumors (50%) carried at least one molecular alteration that is targetable in other tumor types, including alterations in CDKN2A (6.0% biallelically inactivated), ERBB2 (9.3%) and PIK3CA (10%). Immunohistochemistry results correlated well with NGS results for HER2 and p53: Pearson r = 0.82 and 0.83, respectively. As half of GBC patients carry at least one potentially actionable molecular alteration, molecular testing may open the way to explore targeted therapy options for GBC patients.
© 2022. The Author(s).
Conflict of interest statement
Dr. Rachel S. van der Post participated in advisory board meetings of Bristol Myers Squibb (2021) and HER2 testing in gastric cancer (2021). Prof. dr. Marjolijn J.L. Ligtenberg participates in advisory boards of Astra Zeneca, Roche, Bayer, Merck Sharp & Dohme B.V., Jansen-Cilag B.V., Bristol-Myers Squibb and Lilly. Prof. dr. Carla M.L. van Herpen participates in advisory boards of Bayer, Bristol-Myers Squibb, Ipsen, MSD and Regeneron and received research grants, outside the submitted work, from Astra-Zeneca, Bristol-Myers Squibb, MSD, Merck, Ipsen, Novartis, and Sanofi. All other authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
