

Closed-loop vagus nerve stimulation for heart rate control evaluated in the Langendorff-perfused rabbit heart
- PMID: 36335207
- PMCID: PMC9637096
- DOI: 10.1038/s41598-022-23407-2
Closed-loop vagus nerve stimulation for heart rate control evaluated in the Langendorff-perfused rabbit heart
Abstract
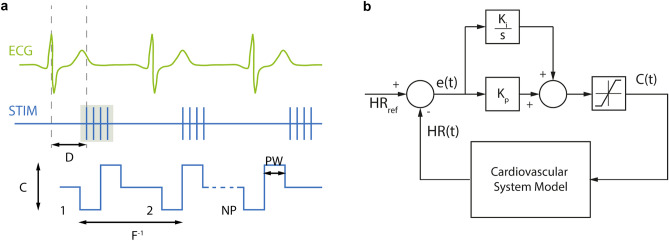
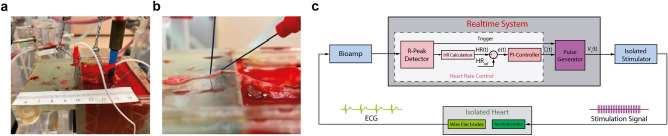
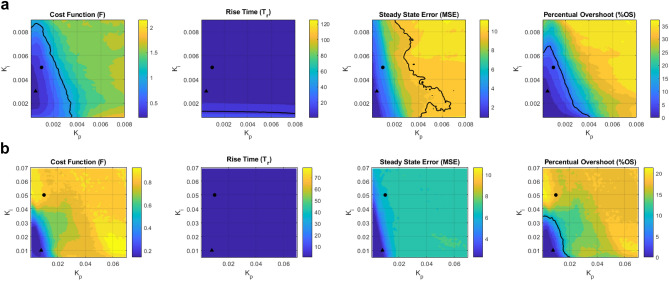
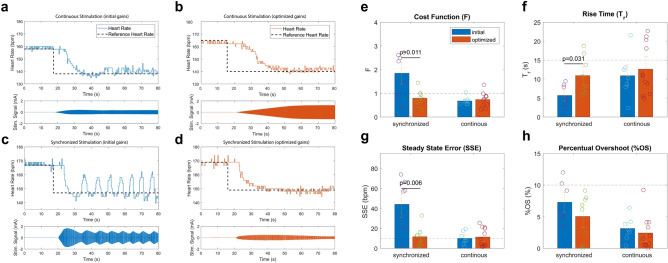
Persistent sinus tachycardia substantially increases the risk of cardiac death. Vagus nerve stimulation (VNS) is known to reduce the heart rate, and hence may be a non-pharmacological alternative for the management of persistent sinus tachycardia. To precisely regulate the heart rate using VNS, closed-loop control strategies are needed. Therefore, in this work, we developed two closed-loop VNS strategies using an in-silico model of the cardiovascular system. Both strategies employ a proportional-integral controller that operates on the current amplitude. While one control strategy continuously delivers stimulation pulses to the vagus nerve, the other applies bursts of stimuli in synchronization with the cardiac cycle. Both were evaluated in Langendorff-perfused rabbit hearts (n = 6) with intact vagal innervation. The controller performance was quantified by rise time (Tr), steady-state error (SSE), and percentual overshoot amplitude (%OS). In the ex-vivo setting, the cardiac-synchronized variant resulted in Tr = 10.7 ± 4.5 s, SSE = 12.7 ± 9.9 bpm and %OS = 5.1 ± 3.6% while continuous stimulation led to Tr = 10.2 ± 5.6 s, SSE = 10 ± 6.7 bpm and %OS = 3.2 ± 1.9%. Overall, both strategies produced a satisfying and reproducible performance, highlighting their potential use in persistent sinus tachycardia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
A novel ex-vivo isolated rabbit heart preparation to explore the cardiac effects of cervical and cardiac vagus nerve stimulation.Sci Rep. 2023 Mar 14;13(1):4214. doi: 10.1038/s41598-023-31135-4. Sci Rep. 2023. PMID: 36918673 Free PMC article.
-
Effects of direct sympathetic and vagus nerve stimulation on the physiology of the whole heart--a novel model of isolated Langendorff perfused rabbit heart with intact dual autonomic innervation.Exp Physiol. 2001 May;86(3):319-29. doi: 10.1113/eph8602146. Exp Physiol. 2001. PMID: 11471534
-
Closed-Loop Vagus Nerve Stimulation Based on State Transition Models.IEEE Trans Biomed Eng. 2018 Jul;65(7):1630-1638. doi: 10.1109/TBME.2017.2759667. Epub 2017 Oct 5. IEEE Trans Biomed Eng. 2018. PMID: 28991730
-
Vagus Nerve Stimulation and the Cardiovascular System.Cold Spring Harb Perspect Med. 2020 Feb 3;10(2):a034173. doi: 10.1101/cshperspect.a034173. Cold Spring Harb Perspect Med. 2020. PMID: 31109966 Free PMC article. Review.
-
The strange case of the ear and the heart: The auricular vagus nerve and its influence on cardiac control.Auton Neurosci. 2016 Aug;199:48-53. doi: 10.1016/j.autneu.2016.06.004. Epub 2016 Jun 28. Auton Neurosci. 2016. PMID: 27388046 Review.
Cited by
-
Precision non-invasive brain stimulation: anin silicopipeline for personalized control of brain dynamics.J Neural Eng. 2025 Apr 22;22(2):026061. doi: 10.1088/1741-2552/adb88f. J Neural Eng. 2025. PMID: 39978066 Free PMC article.
-
A closed loop fully automated wireless vagus nerve stimulation system.Sci Rep. 2025 Jul 30;15(1):27856. doi: 10.1038/s41598-025-11159-8. Sci Rep. 2025. PMID: 40739156 Free PMC article.
-
Exploration of cardiac rehabilitation nursing for elderly patients with myocardial infarction based on individualized cardiac rehabilitation.World J Clin Cases. 2024 Jan 16;12(2):256-266. doi: 10.12998/wjcc.v12.i2.256. World J Clin Cases. 2024. PMID: 38313651 Free PMC article.
-
Importance of cardiac-synchronized vagus nerve stimulation parameters on the provoked chronotropic response for different levels of cardiac innervation.Front Physiol. 2024 May 21;15:1379936. doi: 10.3389/fphys.2024.1379936. eCollection 2024. Front Physiol. 2024. PMID: 38835728 Free PMC article.
-
A novel ex-vivo isolated rabbit heart preparation to explore the cardiac effects of cervical and cardiac vagus nerve stimulation.Sci Rep. 2023 Mar 14;13(1):4214. doi: 10.1038/s41598-023-31135-4. Sci Rep. 2023. PMID: 36918673 Free PMC article.
References
-
- Umana E, Solares CA, Alpert MA. Tachycardia-induced cardiomyopathy. Am. J. Med. 2003;114:51–55. - PubMed
-
- Gupta S, Figueredo VM. Tachycardia mediated cardiomyopathy: Pathophysiology, mechanisms, clinical features and management. Int. J. Cardiol. 2014;172:40–46. - PubMed
-
- Kugler JD, et al. Improvement of left ventricular dysfunction after control of persistent tachycardia. J. Pediatr. 1984;105:543–548. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
