

Perinatal outcomes associated with ICP in twin pregnancies were worse than singletons: an almost 5-year retrospective cohort study
- PMID: 36335293
- PMCID: PMC9636774
- DOI: 10.1186/s12884-022-05160-6
Perinatal outcomes associated with ICP in twin pregnancies were worse than singletons: an almost 5-year retrospective cohort study
Abstract
Background: Intrahepatic cholestasis of pregnancy (ICP) is associated with an increased risk of adverse perinatal outcomes leading to high perinatal morbidity and mortality. However, few studies have examined twin pregnancies complicated by ICP. To assess the perinatal outcomes of twin pregnancies with ICP, a retrospective cohort study was conducted.
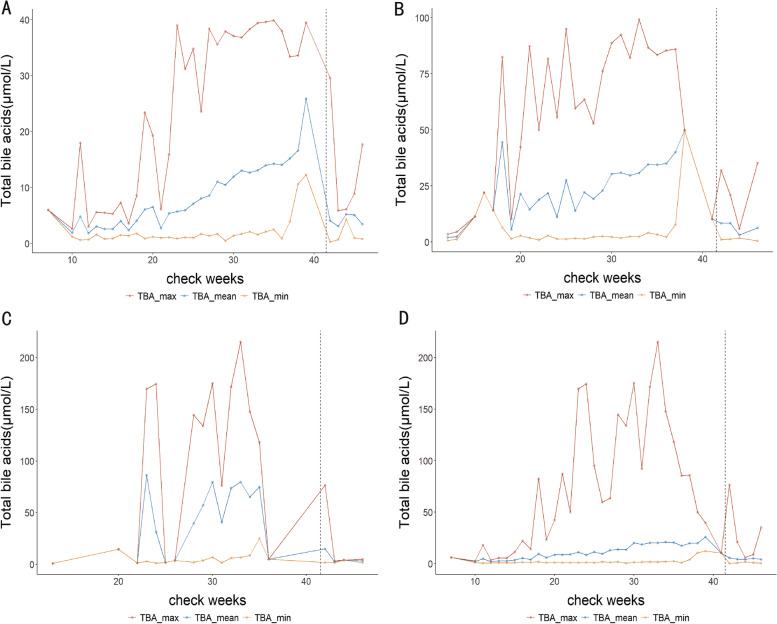
Methods: A total of 633 twin pregnancies and 1267 singleton pregnancies with ICP were included. In addition, a correlation study was performed on the matched total bile acid (TBA) levels from maternal serum, fetal umbilical venous blood, and amniotic fluid of 33 twin pregnancies from twin groups.
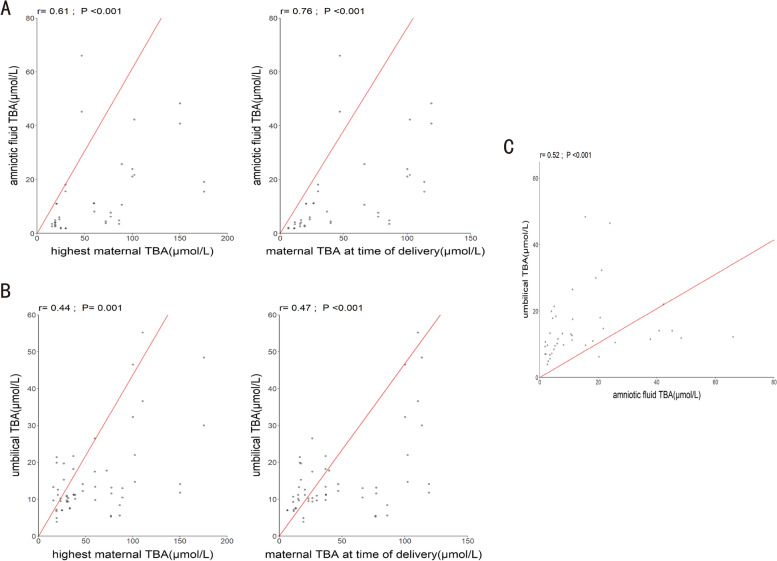
Results: When compared to singletons, twin pregnancies with ICP had a higher risk of cesarean section (CS) (96.4% vs. 76.1%), preterm birth (PTB) (82.6% vs. 19.7%), fetal distress (2.0% vs. 1.3%), and neonatal intensive care unit (NICU) admission (23.6% vs. 5.1%), which was significantly related to increasing TBA levels (P < 0.05). In twin pregnancies with TBA ≥100 μmol/L, the incidences of CS, PTB, fetal distress, neonatal asphyxia, and meconium-stained amniotic fluid were 94.4, 100, 11.1, 5.6, and 36.1%, respectively. Furthermore, the maximum maternal TBA levels were positively correlated with TBA levels in the amniotic fluid (r = 0.61, P < 0.05) and umbilical cord blood (r = 0.44, P < 0.05), and a similar correlation was found for maternal TBA levels at delivery. TBA levels in umbilical cord blood and amniotic fluid also had a significant and positive correlation (r = 0.52, P < 0.05).
Conclusions: Twin pregnancies with ICP had a higher risk for adverse perinatal outcomes than singletons, which was associated with higher TBA levels. TBA can be transported through the placenta and is involved in uterus-placenta-fetal circulation.
Keywords: Intrahepatic cholestasis of pregnancy; Perinatal outcomes; Retrospective cohort study; Twin pregnancies.
© 2022. The Author(s).
Conflict of interest statement
The authors have no actual or potential conflicts of interest to declare. All the funding bodies took part in the design of the study and collection, analysis, and interpretation of data, and the writing of the manuscript.
Figures
Similar articles
-
Preterm birth and stillbirth: total bile acid levels in intrahepatic cholestasis of pregnancy and outcomes of twin pregnancies: a retrospective cohort study from 2014 to 2022.BMC Pregnancy Childbirth. 2025 May 19;25(1):588. doi: 10.1186/s12884-025-07644-7. BMC Pregnancy Childbirth. 2025. PMID: 40389846 Free PMC article.
-
Risk-stratified management strategies for intrahepatic cholestasis of pregnancy: A tertiary center population review over nearly 5 years.Int J Gynaecol Obstet. 2024 Jan;164(1):219-226. doi: 10.1002/ijgo.14987. Epub 2023 Jul 20. Int J Gynaecol Obstet. 2024. PMID: 37470272
-
Perinatal death by bile acid levels in intrahepatic cholestasis of pregnancy: a systematic review.J Matern Fetal Neonatal Med. 2021 Nov;34(21):3614-3622. doi: 10.1080/14767058.2019.1685965. Epub 2019 Nov 19. J Matern Fetal Neonatal Med. 2021. PMID: 31744346
-
Predictors of adverse perinatal outcomes in intrahepatic cholestasis of pregnancy with dichorionic diamniotic twin pregnancies.J Matern Fetal Neonatal Med. 2019 Feb;32(3):472-476. doi: 10.1080/14767058.2017.1384461. Epub 2017 Oct 11. J Matern Fetal Neonatal Med. 2019. PMID: 29020816
-
Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses.Lancet. 2019 Mar 2;393(10174):899-909. doi: 10.1016/S0140-6736(18)31877-4. Epub 2019 Feb 14. Lancet. 2019. PMID: 30773280 Free PMC article.
Cited by
-
A retrospective cohort study on perinatal outcomes of monochorionic and dichorionic twin pregnancies complicated by intrahepatic cholestasis of pregnancy.Sci Rep. 2025 Jul 17;15(1):25984. doi: 10.1038/s41598-025-09792-4. Sci Rep. 2025. PMID: 40676023 Free PMC article.
-
Azathioprine Associated with Intrahepatic Cholestasis in a Patient with Twin Pregnancy after a Second Kidney Transplant.Eur J Case Rep Intern Med. 2024 Mar 11;11(4):004385. doi: 10.12890/2024_004385. eCollection 2024. Eur J Case Rep Intern Med. 2024. PMID: 38584904 Free PMC article.
References
-
- Sharma AV, John S. StatPearls. StatPearls Publishing; 2019. Liver disease in pregnancy. - PubMed
-
- Bacq Y. Liver diseases unique to pregnancy: a 2010 update. Clin Res Hepatol Gastroenterol. 2011;35(3):182–193. - PubMed
-
- Williamson C, Geenes V. Intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2014;124(1):120–133. - PubMed
-
- Berg B, Helm G, Petersohn L, Tryding N. Cholestasis of pregnancy. Clinical and laboratory studies. Acta Obstet Gynecol Scand. 1986;65(2):107–113. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
