

Treatment Time and In-Hospital Mortality Among Patients With ST-Segment Elevation Myocardial Infarction, 2018-2021
- PMID: 36335474
- PMCID: PMC9638953
- DOI: 10.1001/jama.2022.20149
Treatment Time and In-Hospital Mortality Among Patients With ST-Segment Elevation Myocardial Infarction, 2018-2021
Abstract
Importance: Recognizing the association between timely treatment and less myocardial injury for patients with ST-segment elevation myocardial infarction (STEMI), US national guidelines recommend specific treatment-time goals.
Objective: To describe these process measures and outcomes for a recent cohort of patients.
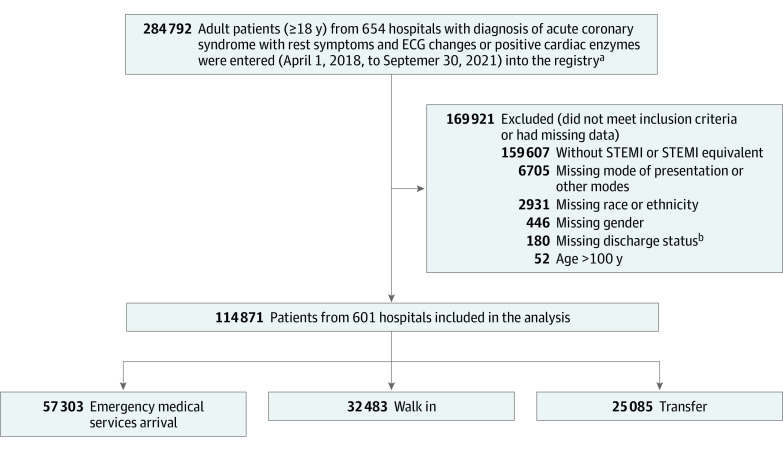
Design, setting, and participants: Cross-sectional study of a diagnosis-based registry between the second quarter of 2018 and the third quarter of 2021 for 114 871 patients with STEMI treated at 648 hospitals in the Get With The Guidelines-Coronary Artery Disease registry.
Exposures: STEMI or STEMI equivalent.
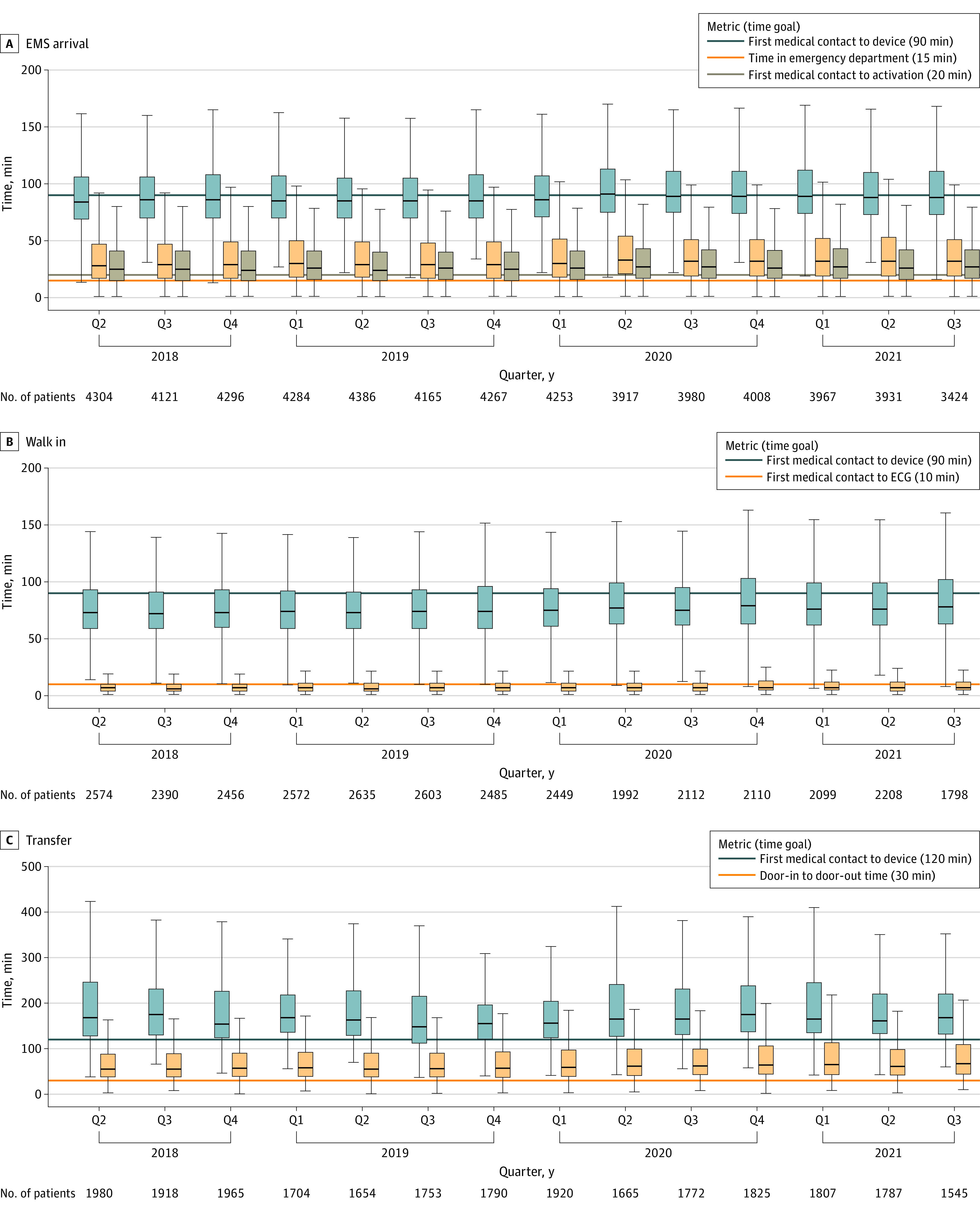
Main outcomes and measures: Treatment times, in-hospital mortality, and adherence to system goals (75% treated ≤90 minutes of first medical contact if the first hospital is percutaneous coronary intervention [PCI]-capable and ≤120 minutes if patients require transfer to a PCI-capable hospital).
Results: In the study population, median age was 63 (IQR, 54-72) years, 71% were men, and 29% were women. Median time from symptom onset to PCI was 148 minutes (IQR, 111-226) for patients presenting to PCI-capable hospitals by emergency medical service, 195 minutes (IQR, 127-349) for patients walking in, and 240 minutes (IQR, 166-402) for patients transferred from another hospital. Adjusted in-hospital mortality was lower for those treated within target times vs beyond time goals for patients transported via emergency medical services (first medical contact to laboratory activation ≤20 minutes [in-hospital mortality, 3.6 vs 9.2] adjusted OR, 0.54 [95% CI, 0.48-0.60], and first medical contact to device ≤90 minutes [in-hospital mortality, 3.3 vs 12.1] adjusted OR, 0.40 [95% CI, 0.36-0.44]), walk-in patients (hospital arrival to device ≤90 minutes [in-hospital mortality, 1.8 vs 4.7] adjusted OR, 0.47 [95% CI, 0.40-0.55]), and transferred patients (door-in to door-out time <30 minutes [in-hospital mortality, 2.9 vs 6.4] adjusted OR, 0.51 [95% CI, 0.32-0.78], and first hospital arrival to device ≤120 minutes [in-hospital mortality, 4.3 vs 14.2] adjusted OR, 0.44 [95% CI, 0.26-0.71]). Regardless of mode of presentation, system goals were not met in most quarters, with the most delayed system performance among patients requiring interhospital transfer (17% treated ≤120 minutes).
Conclusions and relevance: This study of patients with STEMI included in a US national registry provides information on changes in process and outcomes between 2018 and 2021.
Conflict of interest statement
Figures
Comment in
-
Time to Treatment in ST-Segment Elevation Myocardial Infarction: Identifying Dangerous Delays or Diminishing Returns?JAMA. 2022 Nov 22;328(20):2016-2017. doi: 10.1001/jama.2022.19441. JAMA. 2022. PMID: 36335507 No abstract available.
References
-
- Jollis JG, Roettig ML, Aluko AO, et al. ; Reperfusion of Acute Myocardial Infarction in North Carolina Emergency Departments (RACE) Investigators . Implementation of a statewide system for coronary reperfusion for ST-segment elevation myocardial infarction. JAMA. 2007;298(20):2371-2380. doi: 10.1001/jama.298.20.joc70124 - DOI - PubMed
-
- Antman EM, Hand M, Armstrong PW, et al. 2007 Focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2008;117(2):296-329. doi: 10.1161/CIRCULATIONAHA.107.188209 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
