

Characteristics of pulsed electric field cardiac ablation porcine treatment zones with a focal catheter
- PMID: 36335638
- PMCID: PMC10100505
- DOI: 10.1111/jce.15734
Characteristics of pulsed electric field cardiac ablation porcine treatment zones with a focal catheter
Abstract
Objectives: Pulsed electric field (PEF) therapies employ punctuated energy delivery to kill cells in a volume of tissue through mechanisms that are not dependent on thermal processes. A key component to successful cardiac ablation procedures is ensuring the generation of transmural, contiguous ablation zones, which requires in-depth knowledge regarding treatment sizes for a given therapeutic application.
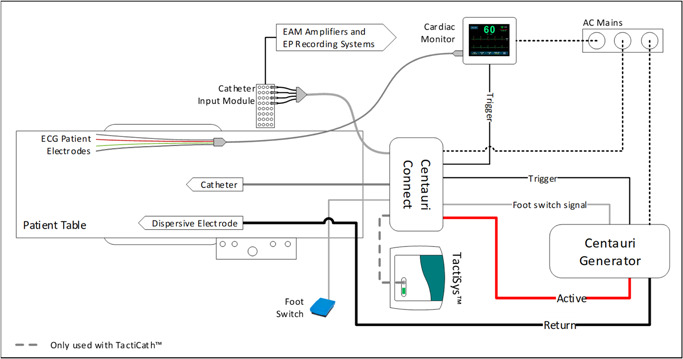
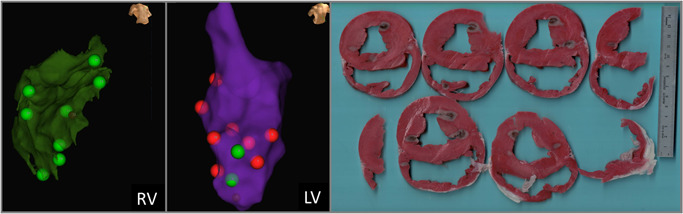
Methods: In this study, a series of acute treatments were delivered to porcine ventricles, where triphenyl tetrazolium chloride (TTC) vitality stain was used to identify treatment effect sizes for the three focal monopolar CENTAURI PEF cardiac ablation energy settings.
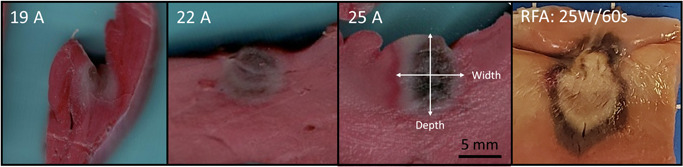
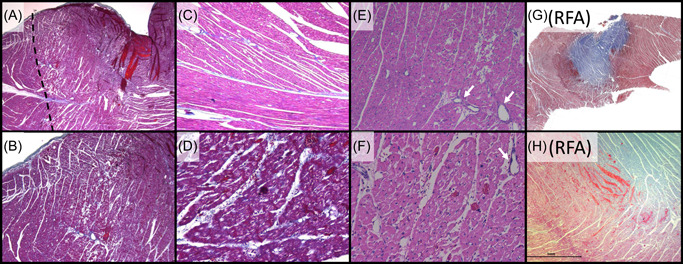
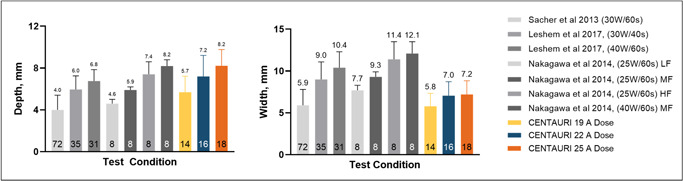
Results: Treatment depths were 5.7, 7.2, and 8.2 mm for the 19, 22, and 25 A energy settings, respectively. Gross pathology indicated umbral zones of hemorrhage surrounded by pale avital TTC-negative-negative tissue, which contrasted significantly from radiofrequency ablation (RF) controls. Histologically, treatment zones are identified by regions of contraction band necrosis and cardiomyocytolysis, which contrasted with RF control lesions composed primarily of coagulation necrosis.
Conclusions: Together, these data indicate the ability for focal monopolar PEF treatments to generate deep treatment zones in cardiac ablation without incurring the gross or histological coagulative characteristics of RF thermal lesions.
Keywords: Aliya; CENTAURI; dose; electroporation; lesion; size.
© 2022 The Authors. Journal of Cardiovascular Electrophysiology published by Wiley Periodicals LLC.
Conflict of interest statement
Dr. Verma reports grants from Bayer, Biosense Webster, Abbott, and Medtronic; advisory for Biosense Webster, Medtronic, Boston Scientific, Adagio Medical, Medlumics, and Ablacon; research with Galaxy Medical. Drs. Neal, Vachani, and Evans are researchers with Galaxy Medical. Dr. Deneke reports advisory for Galaxy Medical and Farapulse; Dr. Nakagawa reports research for Biosense Webster, Galaxy Medical.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
