

A Randomized Controlled Trial Comparing Apixaban With the Vitamin K Antagonist Phenprocoumon in Patients on Chronic Hemodialysis: The AXADIA-AFNET 8 Study
- PMID: 36335915
- PMCID: PMC9875840
- DOI: 10.1161/CIRCULATIONAHA.122.062779
A Randomized Controlled Trial Comparing Apixaban With the Vitamin K Antagonist Phenprocoumon in Patients on Chronic Hemodialysis: The AXADIA-AFNET 8 Study
Abstract
Background: Non-vitamin K oral anticoagulants have become the standard therapy for preventing stroke and ischemic thromboembolism in most patients with atrial fibrillation (AF). The effectiveness and safety of non-vitamin K oral anticoagulants in patients on hemodialysis is not well known.
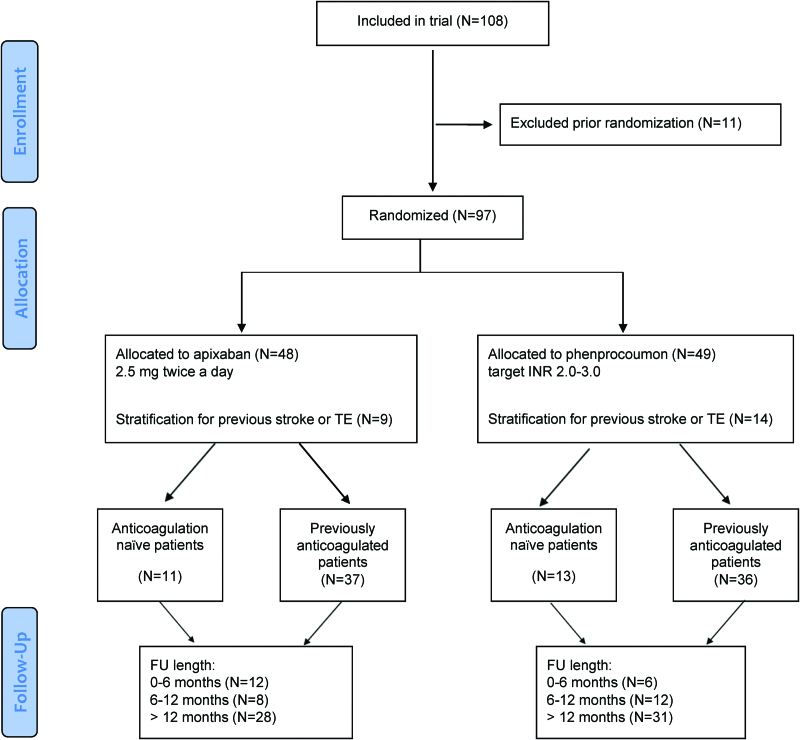
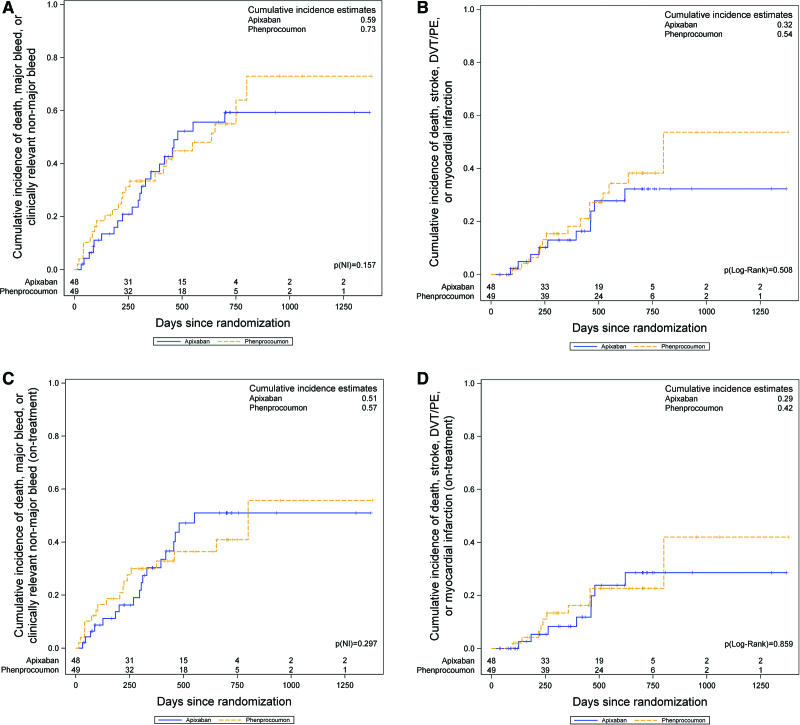
Methods: From June 2017 through May 2022, AXADIA-AFNET 8 (Compare Apixaban and Vitamin K Antagonists in Patients With Atrial Fibrillation and End-Stage Kidney Disease), an investigator-initiated PROBE (prospective randomized open blinded end point) outcome assessment trial, randomized patients with AF on chronic hemodialysis to either apixaban (2.5 mg BID) or the vitamin K antagonist (VKA) phenprocoumon (international normalized ratio, 2.0 to 3.0). The composite primary safety outcome was defined by a first event of major bleeding, clinically relevant nonmajor bleeding, or all-cause death. The primary efficacy outcome was a composite of ischemic stroke, all-cause death, myocardial infarction, and deep vein thrombosis or pulmonary embolism. Our hypothesis was that apixaban is noninferior to VKA.
Results: Thirty-nine sites randomized 97 patients (30% women; mean age 75 years; mean CHA2DS2-VASc [congestive heart failure, hypertension, age ≥75 years, diabetes, stroke or transient ischemic attack, vascular disease, age 65 to 74 years, female sex] score, 4.5; baseline characteristics balanced between groups): 48 to apixaban and 49 to VKA. The median follow-up time was 429 days (range, 37 to 1370) versus 506 days (range, 101 to 1379), respectively. Adherence to apixaban was >80% in 44 of 48 patients; the median time in therapeutic range on VKA was 50.7%. Composite primary safety outcome events occurred in 22 patients (45.8%) on apixaban and in 25 patients (51.0%) on VKA (hazard ratio, 0.93 [95% CI, 0.53-1.65]; Pnoninferiority=0.157). Composite primary efficacy outcome events occurred in 10 patients (20.8%) on apixaban and in 15 patients (30.6%) on VKA (P=0.51; log rank). There were no significant differences regarding individual outcomes (all-cause mortality, 18.8% versus 24.5%; major bleeding, 10.4% versus 12.2%; and myocardial infarction, 4.2% versus 6.1%, respectively).
Conclusions: In this randomized trial comparing apixaban and VKA in patients with AF on hemodialysis with long follow-up, no differences were observed in safety or efficacy outcomes. Even on oral anticoagulation, patients with AF on hemodialysis remain at high risk of cardiovascular events. Larger randomized trials are needed to determine the optimal anticoagulation regimen for patients with AF on hemodialysis.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT02933697.
Keywords: atrial fibrillation; randomized controlled trial; renal dialysis; stroke.
Figures
Comment in
-
Apixaban for stroke prevention in hemodialysis patients with nonvalvular atrial fibrillation.Kidney Int. 2023 Jun;103(6):1014-1017. doi: 10.1016/j.kint.2023.03.027. Epub 2023 Apr 12. Kidney Int. 2023. PMID: 37059362 No abstract available.
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, et al. ; ESC Scientific Document Group. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC): developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612 - PubMed
-
- Steffel J, Collins R, Antz M, Cornu P, Desteghe L, Haeusler KG, Oldgren J, Reinecke H, Roldan-Schilling V, Rowell N, et al. 2021 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace. 2021;23:1612–1676. doi: 10.1093/europace/euab065 - PubMed
-
- Eikelboom JW, Connolly SJ, Brueckmann M, Granger CB, Kappetein AP, Mack MJ, Blatchford J, Devenny K, Friedman J, Guiver K, et al. ; RE-ALIGN Investigators. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med. 2013;369:1206–1214. doi: 10.1056/NEJMoa1300615 - PubMed
-
- Connolly SJ, Karthikeyan G, Ntsekhe M, Haileamlak A, El Sayed A, El Ghamrawy A, Damasceno A, Avezum A, Dans AML, Gitura B, et al. ; INVICTUS Investigators. Rivaroxaban in rheumatic heart disease-associated atrial fibrillation. N Engl J Med. 2022;387:978–988. doi: 10.1056/NEJMoa2209051 - PubMed
-
- Reinecke H, Brand E, Mesters R, Schaebitz WR, Fisher M, Pavenstaedt H, Breithardt G. Dilemmas in the management of atrial fibrillation in chronic kidney disease. J Am Soc Nephrol. 2009;20:705–711. doi: 10.1681/ASN.2007111207 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
