

Survival After Invasive or Conservative Management of Stable Coronary Disease
- PMID: 36335918
- PMCID: PMC9797439
- DOI: 10.1161/CIRCULATIONAHA.122.062714
Survival After Invasive or Conservative Management of Stable Coronary Disease
Abstract
Background: The ISCHEMIA trial (International Study of Comparative Health Effectiveness With Medical and Invasive Approaches) compared an initial invasive versus an initial conservative management strategy for patients with chronic coronary disease and moderate or severe ischemia, with no major difference in most outcomes during a median of 3.2 years. Extended follow-up for mortality is ongoing.
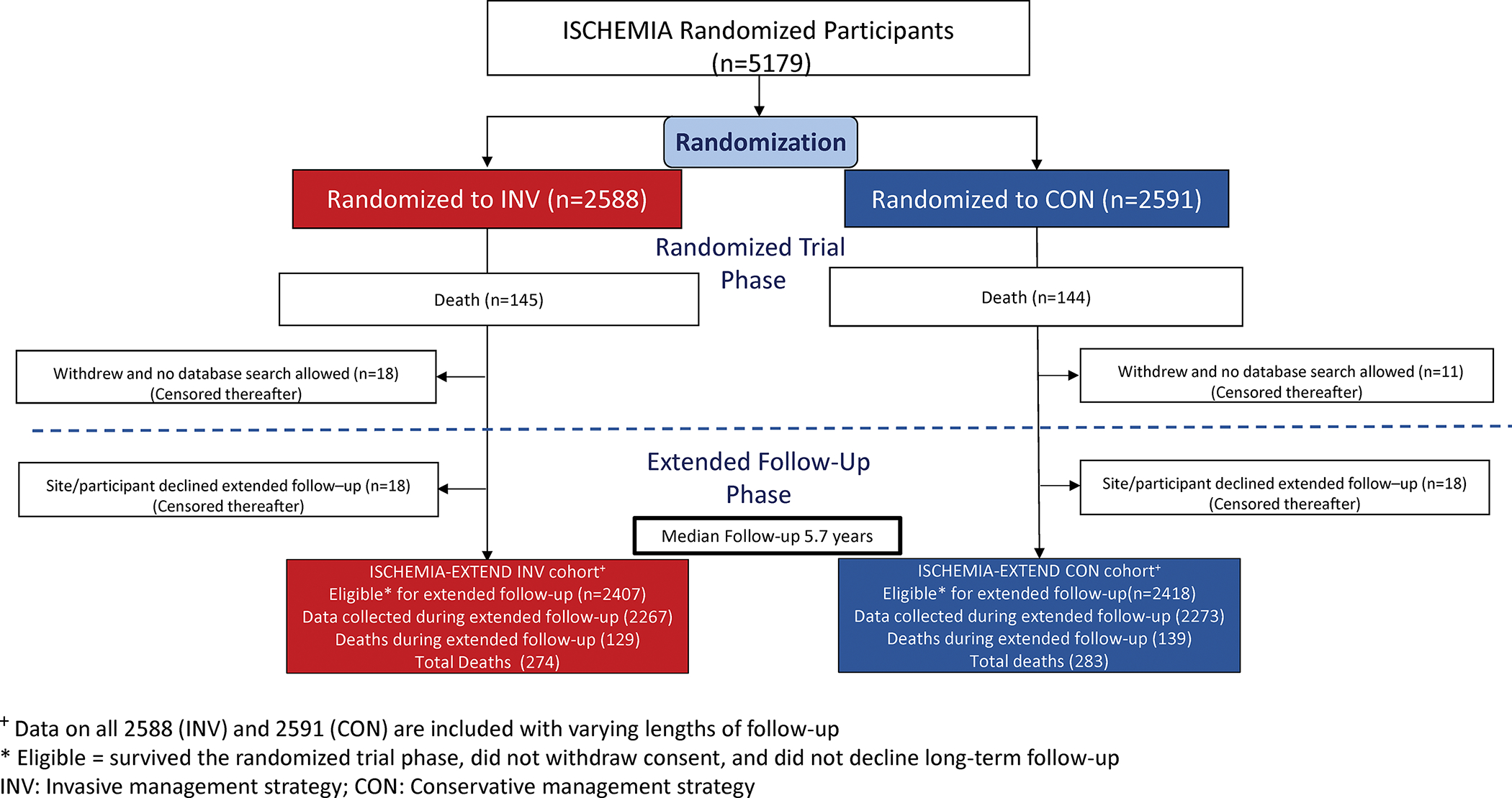
Methods: ISCHEMIA participants were randomized to an initial invasive strategy added to guideline-directed medical therapy or a conservative strategy. Patients with moderate or severe ischemia, ejection fraction ≥35%, and no recent acute coronary syndromes were included. Those with an unacceptable level of angina were excluded. Extended follow-up for vital status is being conducted by sites or through central death index search. Data obtained through December 2021 are included in this interim report. We analyzed all-cause, cardiovascular, and noncardiovascular mortality by randomized strategy, using nonparametric cumulative incidence estimators, Cox regression models, and Bayesian methods. Undetermined deaths were classified as cardiovascular as prespecified in the trial protocol.
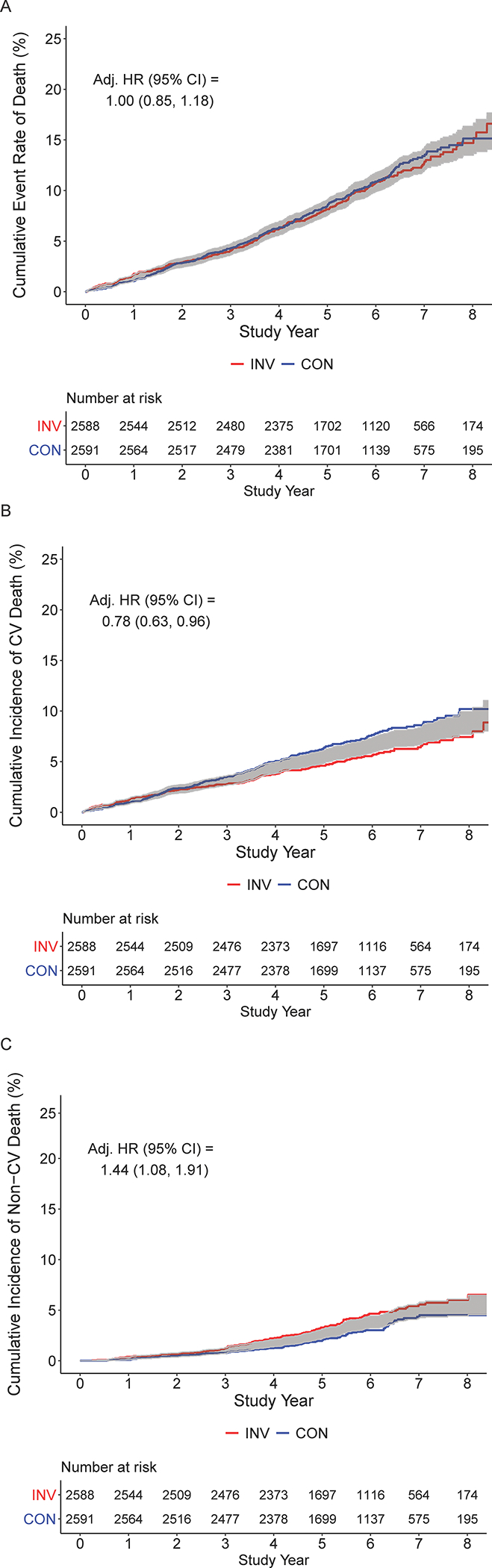
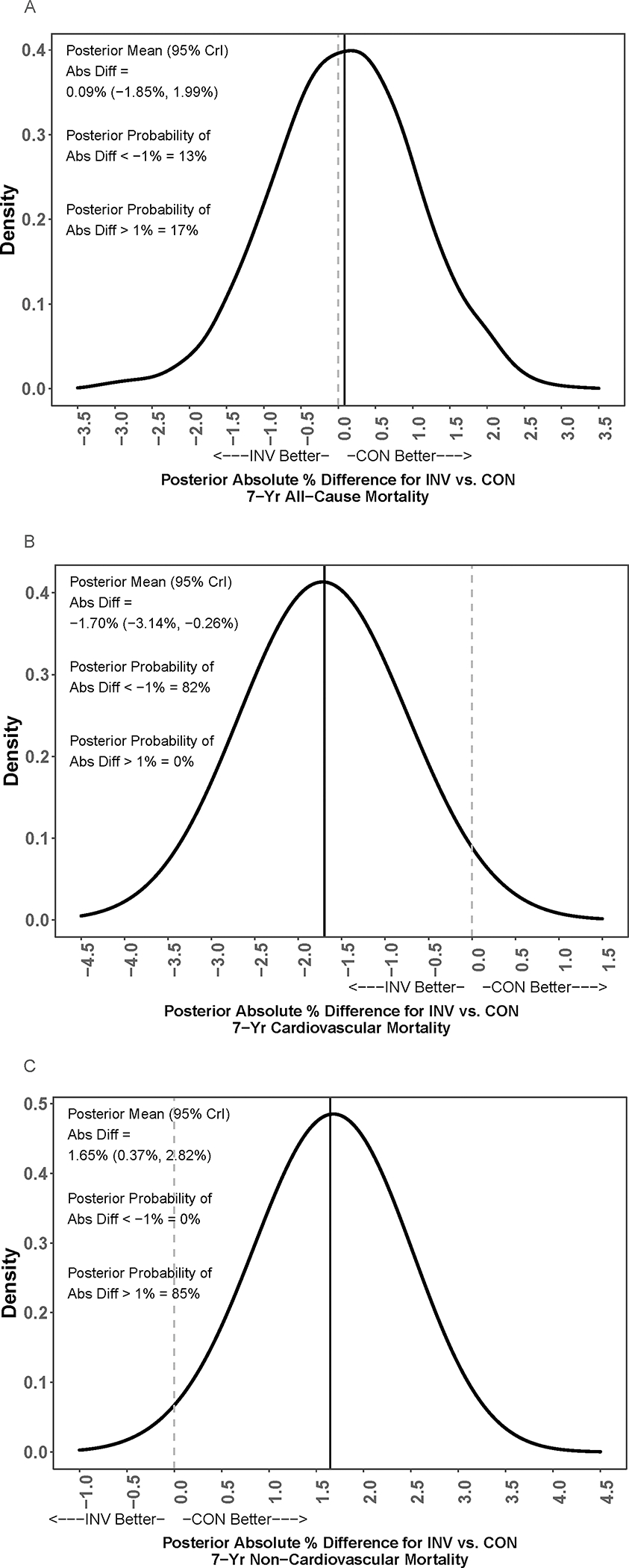
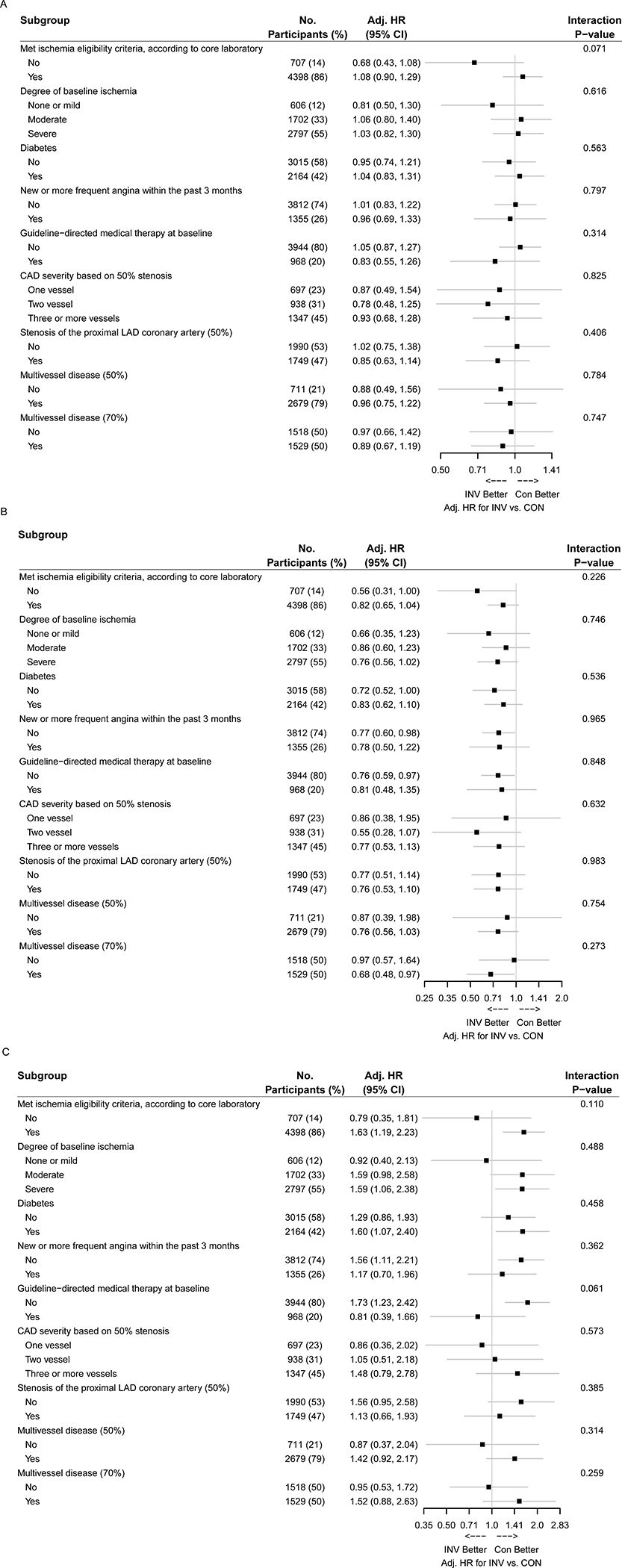
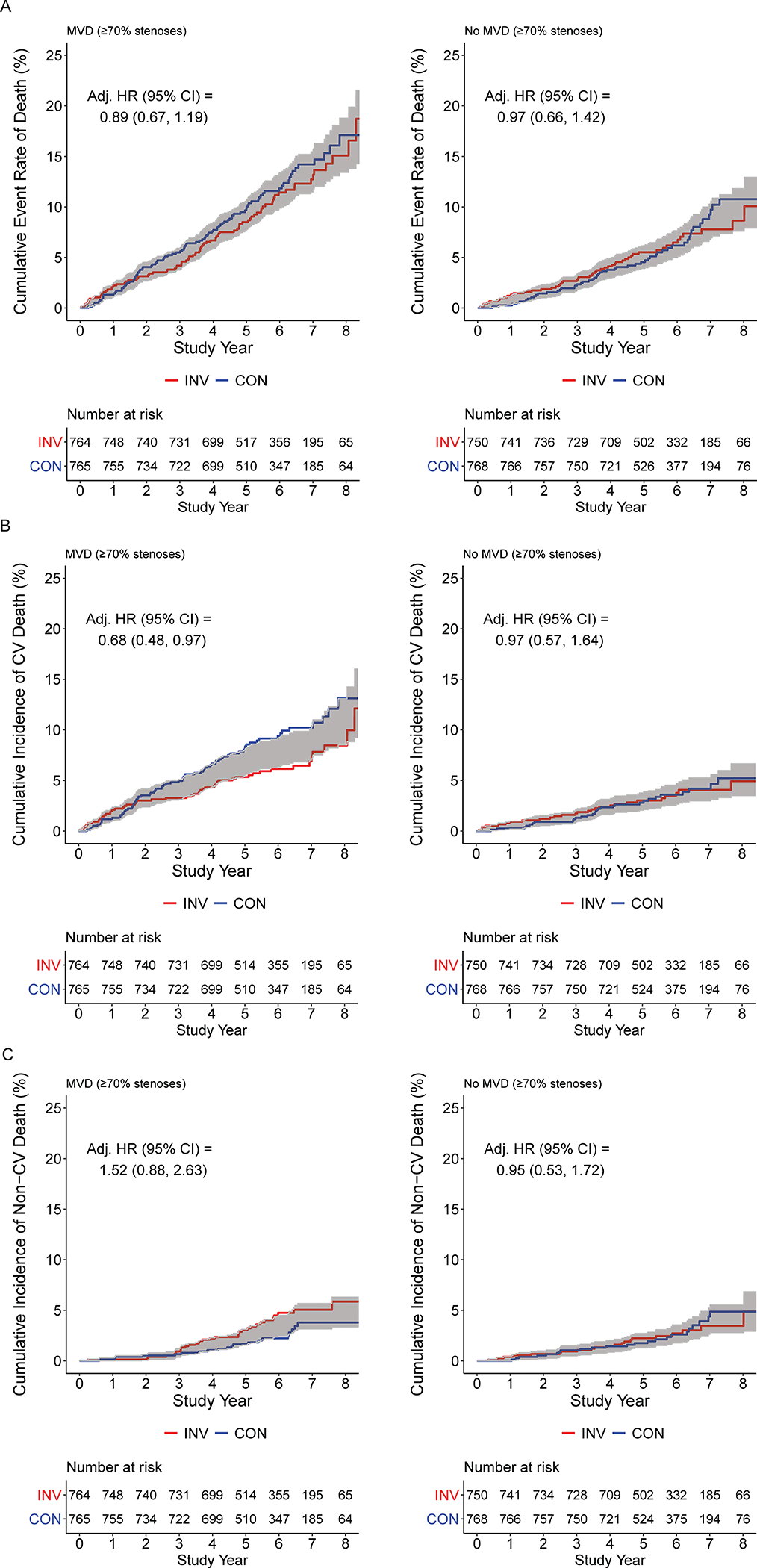
Results: Baseline characteristics for 5179 original ISCHEMIA trial participants included median age 65 years, 23% women, 16% Hispanic, 4% Black, 42% with diabetes, and median ejection fraction 0.60. A total of 557 deaths accrued during a median follow-up of 5.7 years, with 268 of these added in the extended follow-up phase. This included a total of 343 cardiovascular deaths, 192 noncardiovascular deaths, and 22 unclassified deaths. All-cause mortality was not different between randomized treatment groups (7-year rate, 12.7% in invasive strategy, 13.4% in conservative strategy; adjusted hazard ratio, 1.00 [95% CI, 0.85-1.18]). There was a lower 7-year rate cardiovascular mortality (6.4% versus 8.6%; adjusted hazard ratio, 0.78 [95% CI, 0.63-0.96]) with an initial invasive strategy but a higher 7-year rate of noncardiovascular mortality (5.6% versus 4.4%; adjusted hazard ratio, 1.44 [95% CI, 1.08-1.91]) compared with the conservative strategy. No heterogeneity of treatment effect was evident in prespecified subgroups, including multivessel coronary disease.
Conclusions: There was no difference in all-cause mortality with an initial invasive strategy compared with an initial conservative strategy, but there was lower risk of cardiovascular mortality and higher risk of noncardiovascular mortality with an initial invasive strategy during a median follow-up of 5.7 years.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT04894877.
Keywords: catheterization; coronary artery bypass; medication therapy management; myocardial ischemia; percutaneous coronary intervention.
Figures
Comment in
-
If the Fates Allow: The Zero-Sum Game of ISCHEMIA-EXTEND.Circulation. 2023 Jan 3;147(1):20-22. doi: 10.1161/CIRCULATIONAHA.122.063033. Epub 2022 Nov 6. Circulation. 2023. PMID: 36335920 No abstract available.
References
-
- Maron DJ, Hochman JS, O’Brien SM, Reynolds HR, Boden WE, Stone GW, Bangalore S, Spertus JA, Mark DB, Alexander KP, et al. International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial: Rationale and design. American Heart Journal. 2018;201:124–135. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
