

Endotracheal Intubation Strategy, Success, and Adverse Events Among Emergency Department Patients During the COVID-19 Pandemic
- PMID: 36336542
- PMCID: PMC9633323
- DOI: 10.1016/j.annemergmed.2022.09.013
Endotracheal Intubation Strategy, Success, and Adverse Events Among Emergency Department Patients During the COVID-19 Pandemic
Abstract
Study objective: To describe endotracheal intubation practices in emergency departments by staff intubating patients early in the coronavirus disease 2019 (COVID-19) pandemic.
Methods: Multicenter prospective cohort study of endotracheal intubations conducted at 20 US academic emergency departments from May to December 2020, stratified by known or suspected COVID-19 status. We used multivariable regression to measure the association between intubation strategy, COVID-19 known or suspected status, first-pass success, and adverse events.
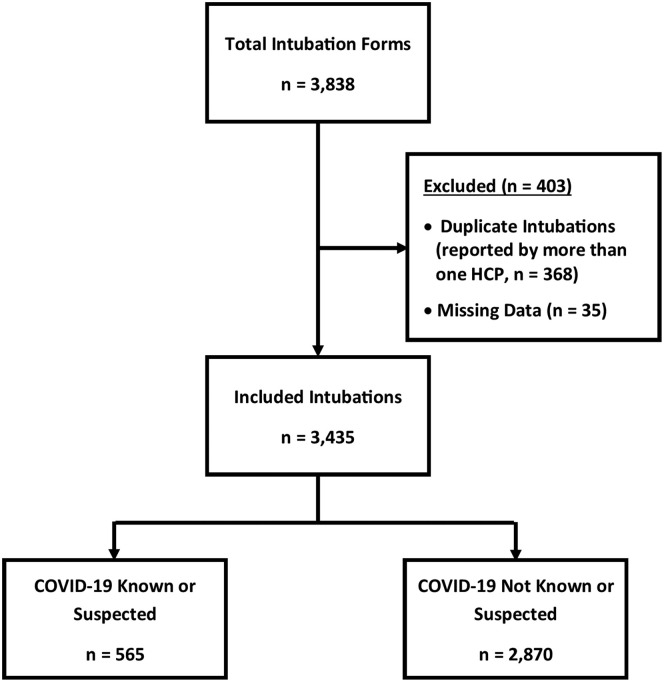
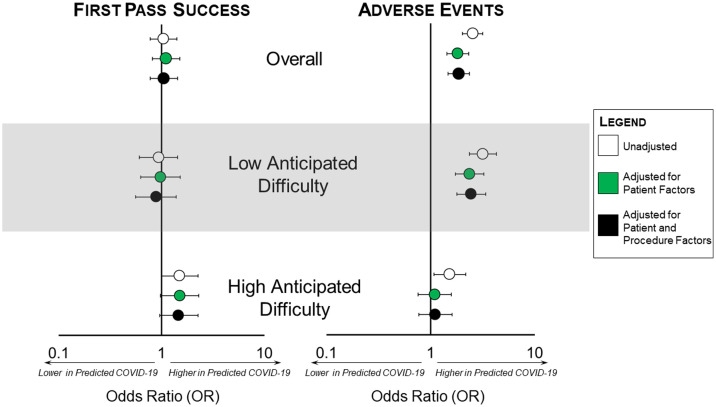
Results: There were 3,435 unique emergency department endotracheal intubations by 586 participating physicians or advanced practice providers; 565 (18%) patients were known or suspected of having COVID-19 at the time of endotracheal intubation. Compared with patients not known or suspected of COVID-19, endotracheal intubations of patients with known or suspected COVID-19 were more often performed using video laryngoscopy (88% versus 82%, difference 6.3%; 95% confidence interval [CI], 3.0% to 9.6%) and passive nasal oxygenation (44% versus 39%, difference 5.1%; 95% CI, 0.9% to 9.3%). First-pass success was not different between those who were and were not known or suspected of COVID-19 (87% versus 86%, difference 0.6%; 95% CI, -2.4% to 3.6%). Adjusting for patient characteristics and procedure factors in those with low anticipated airway difficulty (n=2,374), adverse events (most commonly hypoxia) occurred more frequently in patients with known or suspected COVID-19 (35% versus 19%, adjusted odds ratio 2.4; 95% CI, 1.7 to 3.3).
Conclusion: Compared with patients not known or suspected of COVID-19, endotracheal intubation of those confirmed or suspected to have COVID-19 was associated with a similar first-pass intubation success rate but higher risk-adjusted adverse events.
Copyright © 2022 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
