

Association between hepatic steatosis and fibrosis with measures of insulin sensitivity in patients with severe obesity and type 2 diabetes - a cross-sectional study
- PMID: 36336684
- PMCID: PMC9639281
- DOI: 10.1186/s12876-022-02550-0
Association between hepatic steatosis and fibrosis with measures of insulin sensitivity in patients with severe obesity and type 2 diabetes - a cross-sectional study
Abstract
Background: Obesity, non-alcoholic fatty liver disease (NAFLD) and insulin resistance are three pathological conditions highly correlated, but this relationship is not fully elucidated. Hence, we aimed to assess the association of hepatic steatosis and fibrosis with different measures of insulin sensitivity in patients with severe obesity and type 2 diabetes mellitus (T2DM).
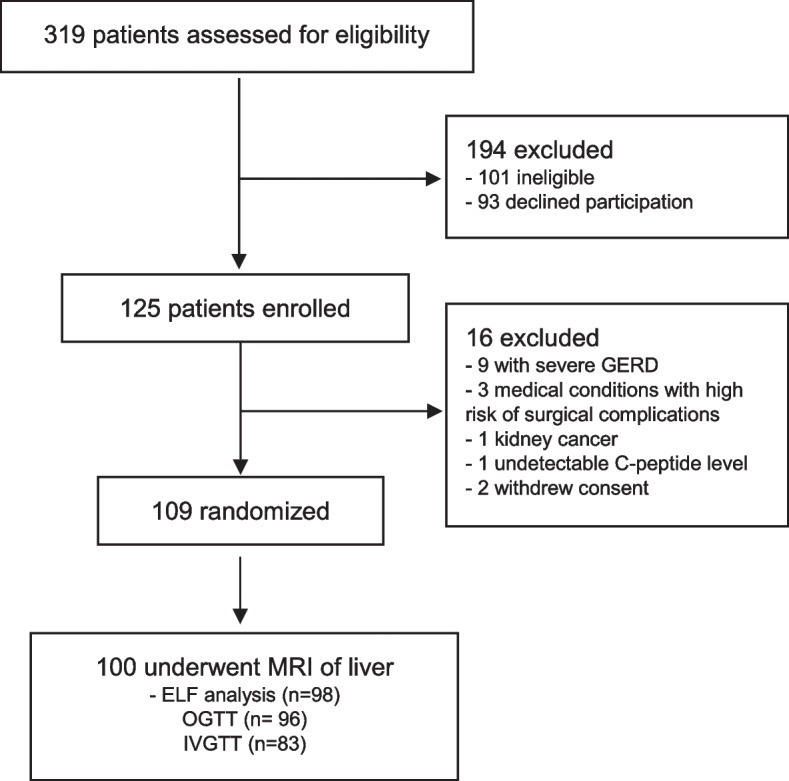
Methods: A cross-sectional study (Oseberg trial) including patients with T2DM referred for bariatric surgery at Vestfold Hospital Trust, Norway. Magnetic resonance imaging (MRI) and the enhanced liver fibrosis (ELF) test was used for estimation of liver fat fraction (LFF) and degree of fibrosis, respectively. Oral and intravenous glucose tolerance tests were applied for estimation of insulin sensitivity (HOMA2S, Matsuda ISI and MinMod SI).
Results: A total of 100 patients (mean [SD] age 47.5 [9.7] years, 65% women, BMI 42.0 [5.3] kg/m2 and 98% with metabolic syndrome) were included in the analyses. The mean (SD) LFF in the total population was 19.1 (11.5), and the mean (SD) ELF score was 8.46 (0.84), a value representing moderate fibrosis. LFF was inversely associated with HOMA2S and Matsuda ISI, and both measures were significantly higher in the no or low-grade steatosis group compared with the medium-to-high grade steatosis group (mean difference [95% CI] 5.9 [2.2-9.6]%, Cohen's d = 0.75), and (0.7 [0.3-1.1], Cohen's d = 0.80, respectively). There was no association between LFF, as a categorical or continuous variable, and MinMod SI. The proportions of patients with none to mild fibrosis, moderate fibrosis and severe fibrosis were 14, 78 and 6%, respectively, and there were no significant associations between level of fibrosis and measures of insulin sensitivity.
Conclusions: Patients with morbid obesity and T2DM demonstrated high levels of liver fat fraction, and we showed that hepatic steatosis, but not the degree of liver fibrosis, was associated with different measures of insulin sensitivity in patients with severe obesity and T2DM. Further, our results might indicate that the LFF is primarily associated with hepatic, and not peripheral insulin sensitivity. To improve the diagnosis of NAFLD and the prediction of its progression, more studies are needed to reveal the pathological mechanistic pathways involved in NAFLD and insulin sensitivity.
Trial registration: ClinicalTrials.gov: NCT01778738.
Keywords: ELF test; Hepatic steatosis; Insulin sensitivity; Liver fat fraction; Liver fibrosis; Severe obesity; Type 2 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. - PubMed
-
- Petroni ML, Brodosi L, Bugianesi E, Marchesini G. Management of non-alcoholic fatty liver disease. BMJ. 2021;372:m4747. - PubMed
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
