

Angiography-derived index of microvascular resistance in takotsubo syndrome
- PMID: 36336756
- PMCID: PMC9813145
- DOI: 10.1007/s10554-022-02698-6
Angiography-derived index of microvascular resistance in takotsubo syndrome
Abstract
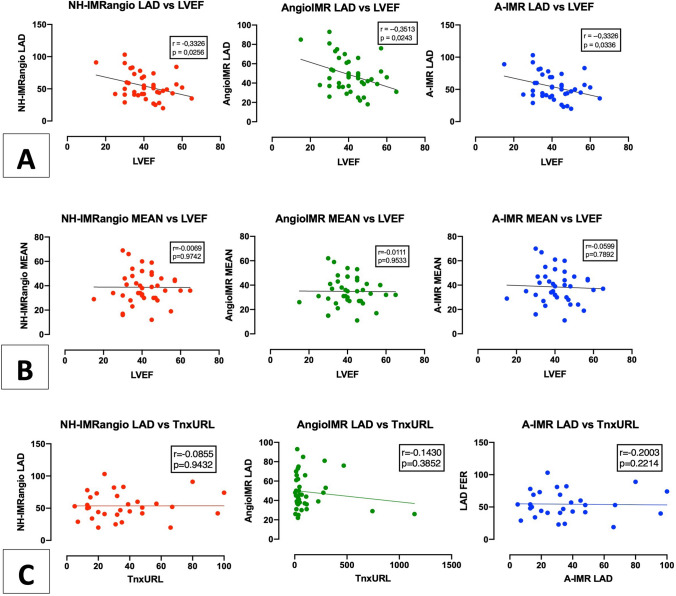
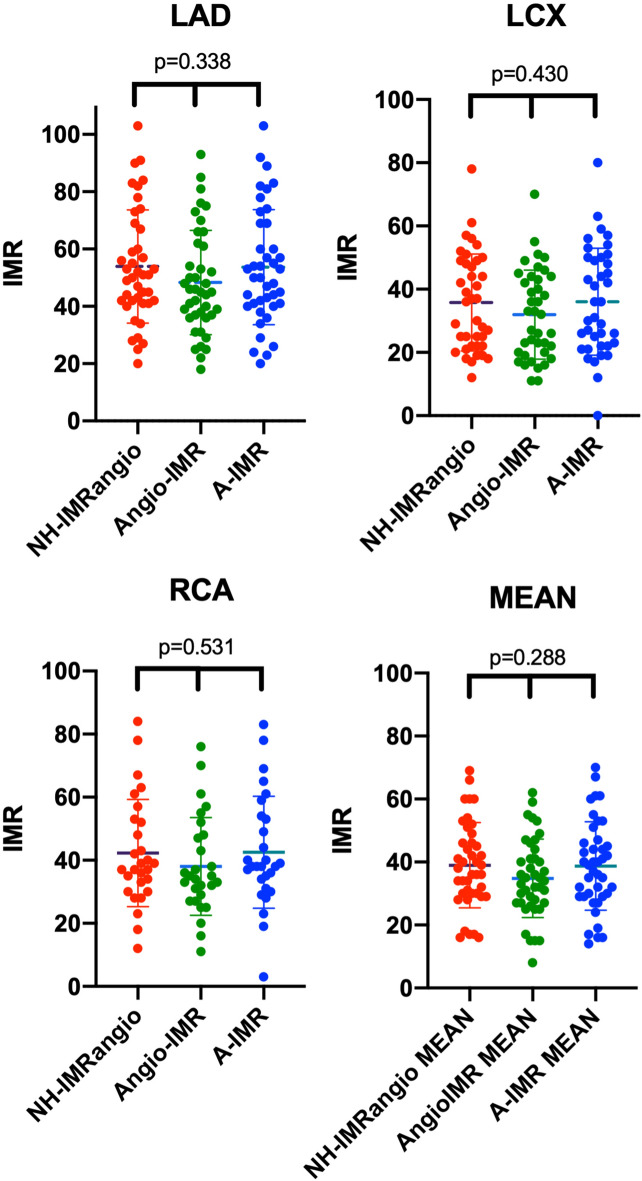
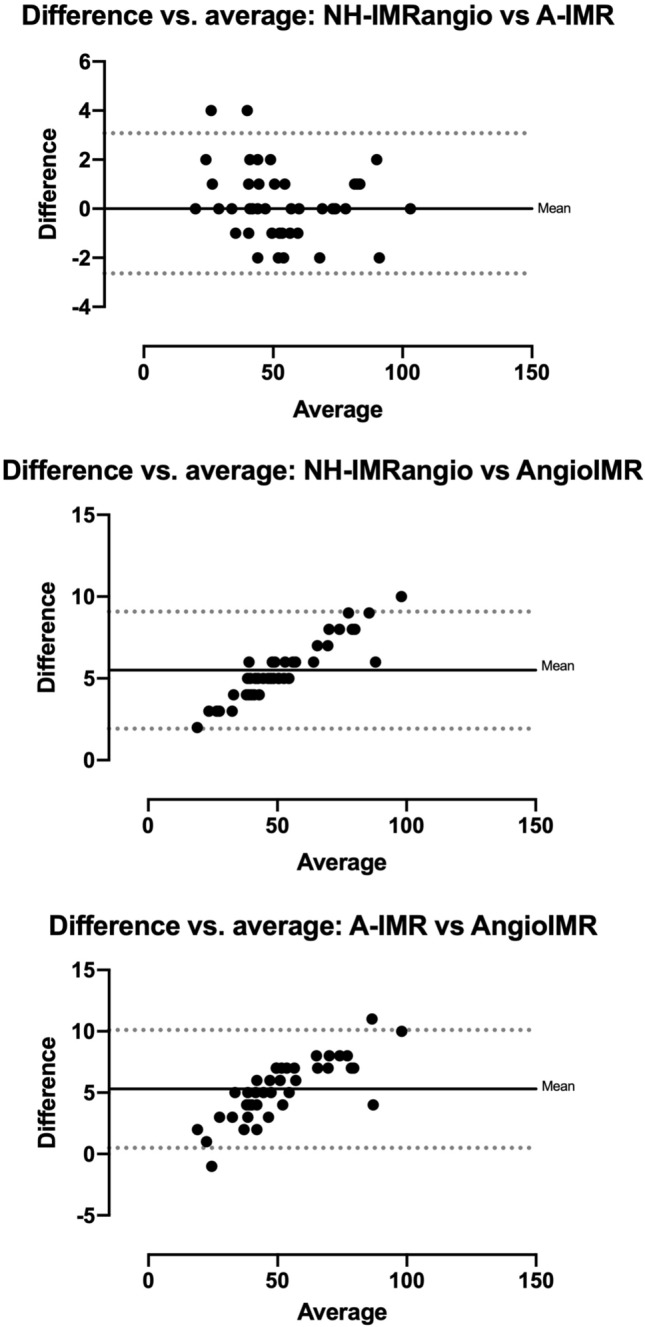
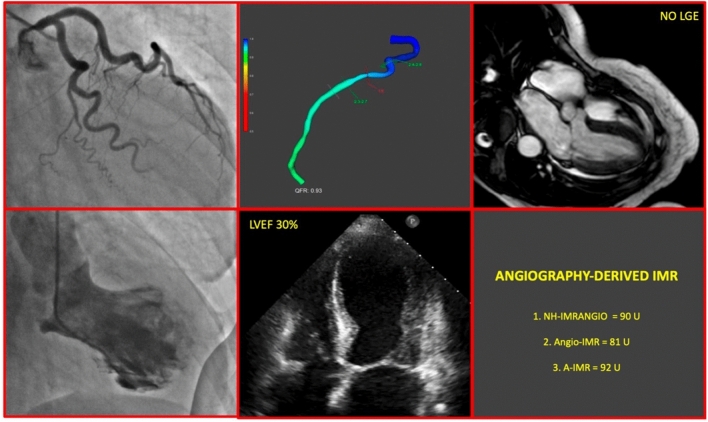
Coronary microvascular dysfunction (CMD) has been proposed as a key driver in the etiopathogenesis of Takotsubo syndrome (TTS), likely related to an "adrenergic storm" upon a susceptible microvascular circulation. The aim of our manuscript was to assess CMD in patients with TTS through the computation of the angiography-derived index of microcirculatory resistance (IMR) and its correlation with clinical presentation. Coronary angiograms of 41 consecutive TTS patients were retrospectively analyzed to derive angiography-based indices of CMD. Three indices (NH-IMRangio, AngioIMR and A-IMR) were calculated based on quantitative flow ratio. CMD was defined as an IMRangio value ≥ 25 units. The correlation between CMD and clinical presentation was then assessed. Median age was 76 years, 85.7% were women and mean left ventricular ejection fraction (LVEF) at first echocardiogram was 41.2%. Angiography-derived IMR was higher in left anterior descending artery (LAD) than circumflex and right coronary artery with either NH-IMRangio (53.9 ± 19.8 vs 35.8 ± 15.4 vs 40.8 ± 18.5, p-value < 0.001), AngioIMR (47.2 ± 17.3 vs 31.8 ± 12.2 vs 37.3 ± 13.7, p-value < 0.001) or A-IMR (52.7 ± 19 vs 36.1 ± 14.1 vs 41.8 ± 16.1, p-value < 0.001). All patients presented CMD with angiography-derived IMR ≥ 25 in at least one territory with each formula. Angiography-derived IMR in LAD territory was significantly higher in patients presenting with LVEF impairment (≤ 40%) than in those with preserved ventricular global function (NH-IMRangio: 59.3 ± 18.1 vs 46.3 ± 16.0 p-value = 0.030; AngioIMR: 52.9 ± 17.8 vs 41.4 ± 14.2, p-value = 0.037; A-IMR: 59.2 ± 18.6 vs 46.3 ± 17.0, p-value = 0.035). CMD assessed with angiography-derived IMR is a common finding in TTS and it is inversely correlated with LV function. The available formulas have a substantial superimposable diagnostic performance in assessing coronary microvascular function.
Keywords: Coronary physiology; Index of microvascular resistance; Quantitative flow ratio; Takotsubo syndrome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
Figures

Comment in
-
Angiography-derived index of microvascular resistance and the pathophysiology of takotsubo syndrome.Int J Cardiovasc Imaging. 2023 Mar;39(3):469-470. doi: 10.1007/s10554-022-02766-x. Epub 2022 Dec 7. Int J Cardiovasc Imaging. 2023. PMID: 36478530 No abstract available.
-
Editor's choice to the January 2023 issue : Angiography-derived index of microvascular resistance in Takotsubo syndrome.Int J Cardiovasc Imaging. 2023 Jan;39(1):1-2. doi: 10.1007/s10554-022-02783-w. Int J Cardiovasc Imaging. 2023. PMID: 36543910 No abstract available.
References
-
- Ghadri JR, Cammann VL, Jurisic S, Seifert B, Napp LC, Diekmann J, et al. A novel clinical score (InterTAK Diagnostic Score) to differentiate takotsubo syndrome from acute coronary syndrome: results from the International Takotsubo Registry. Eur J Heart Fail. 2017;19(8):1036–1042. doi: 10.1002/ejhf.683. - DOI - PubMed
-
- Omerovic E, Citro R, Bossone E, Redfors B, Backs J, Bruns B, et al. Pathophysiology of takotsubo syndrome – a joint scientific statement from the heart failure association takotsubo syndrome study group and myocardial function working group of the european society of cardiology – part 2: vascular pathophysiology, gender and sex hormones, genetics, chronic cardiovascular problems and clinical implications. Eur J Heart Fail. 2021;24(2):274–286. doi: 10.1002/ejhf.2368. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
