

CAD-RADS™ 2.0 - 2022 Coronary Artery Disease - Reporting and Data System An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR) and the North America Society of Cardiovascular Imaging (NASCI)
- PMID: 36339062
- PMCID: PMC9627235
- DOI: 10.1148/ryct.220183
CAD-RADS™ 2.0 - 2022 Coronary Artery Disease - Reporting and Data System An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR) and the North America Society of Cardiovascular Imaging (NASCI)
Abstract
Coronary Artery Disease Reporting and Data System (CAD-RADS) was created to standardize reporting system for patients undergoing coronary CT angiography (CCTA) and to guide possible next steps in patient management. The goal of this updated 2022 CAD-RADS 2.0 is to improve the initial reporting system for CCTA by considering new technical developments in Cardiac CT, including data from recent clinical trials and new clinical guidelines. The updated CAD-RADS classification will follow an established framework of stenosis, plaque burden, and modifiers, which will include assessment of lesion-specific ischemia using CT fractional-flow-reserve (CT-FFR) or myocardial CT perfusion (CTP), when performed. Similar to the method used in the original CAD-RADS version, the determinant for stenosis severity classification will be the most severe coronary artery luminal stenosis on a per-patient basis, ranging from CAD-RADS 0 (zero) for absence of any plaque or stenosis to CAD-RADS 5 indicating the presence of at least one totally occluded coronary artery. Given the increasing data supporting the prognostic relevance of coronary plaque burden, this document will provide various methods to estimate and report total plaque burden. The addition of P1 to P4 descriptors are used to denote increasing categories of plaque burden. The main goal of CAD-RADS, which should always be interpreted together with the impression found in the report, remains to facilitate communication of test results with referring physicians along with suggestions for subsequent patient management. In addition, CAD-RADS will continue to provide a framework of standardization that may benefit education, research, peer-review, artificial intelligence development, clinical trial design, population health and quality assurance with the ultimate goal of improving patient care. Keywords: Coronary Artery Disease, Coronary CTA, CAD-RADS, Reporting and Data System, Stenosis Severity, Report Standardization Terminology, Plaque Burden, Ischemia Supplemental material is available for this article. This article is published synchronously in Radiology: Cardiothoracic Imaging, Journal of Cardiovascular Computed Tomography, JACC: Cardiovascular Imaging, Journal of the American College of Radiology, and International Journal for Cardiovascular Imaging. © 2022 Society of Cardiovascular Computed Tomography. Published by RSNA with permission.
Keywords: CAD-RADS; Coronary Artery Disease; Coronary CTA; Ischemia; Plaque Burden; Report Standardization Terminology; Reporting and Data System; Stenosis Severity.
© 2022 by the Radiological Society of North America, Inc.
Conflict of interest statement
Declaration of competing interest :*In accordance with SCCT policy, writing group members and reviewers are required to disclose relationships with industry; see Appendices 1 and 2 for detailed information.
Figures
![Timeline plots of total quarterly PubMed citations resulting from the
search “CAD-RADS” [Title/Abstract] OR “CADRADS”
[Title/Abstract]. The date of the search was January 25, 2021. Permission
received (63). Radiol Cardiothorac Imaging. 2021 Jun; 3 (3): e210016.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/ae9d/9627235/13b11d24ebfe/ryct.220183.fig1.jpg)
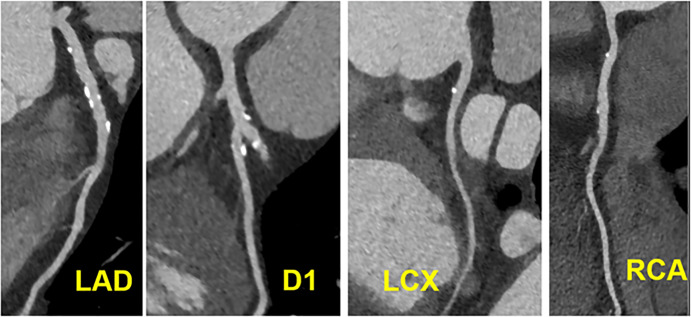
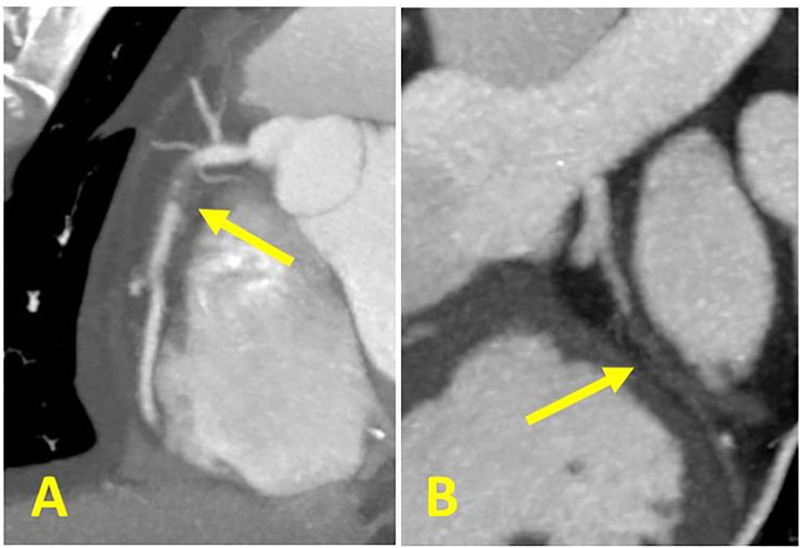


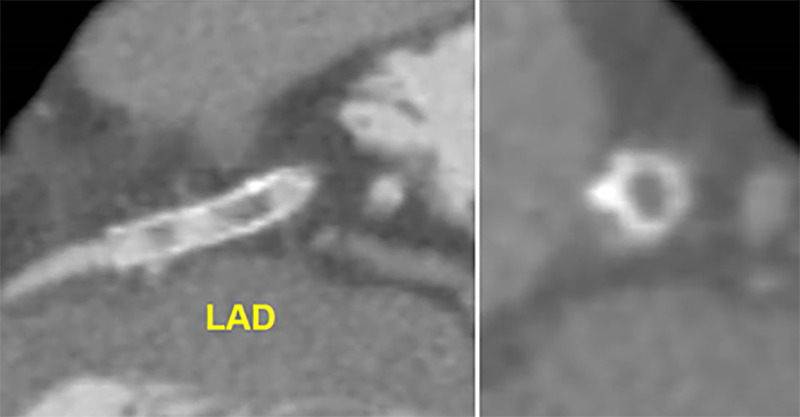

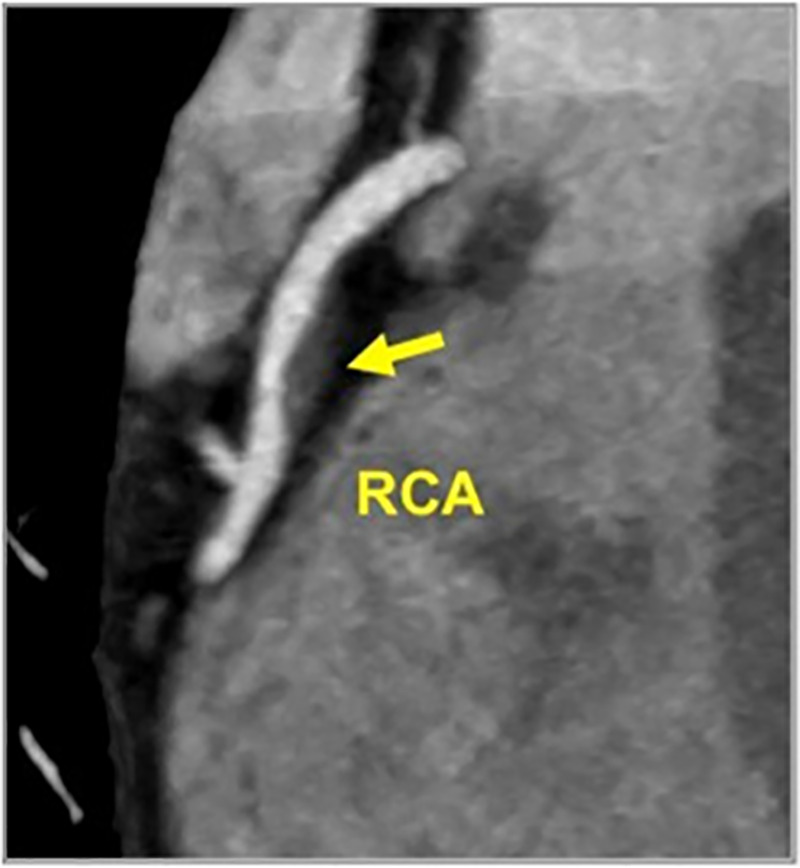
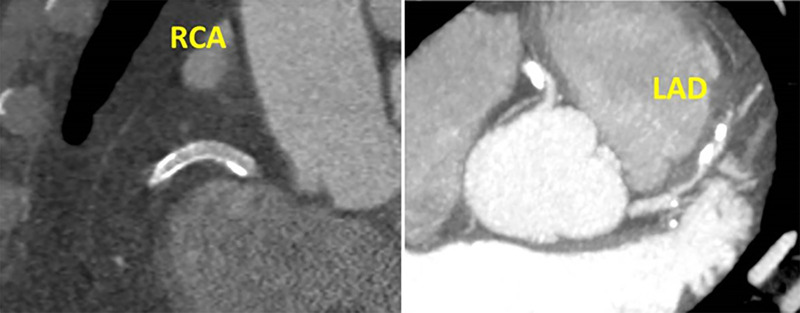
![High-risk plaque (HRP) features on coronary CTA. (A) Spotty calcium,
defined as punctate calcium within a plaque (B) “napkin ring
sign,” defined in a non-calcified plaque cross-sectional image by the
presence of two features: a central area of low attenuation plaque that is
apparently in contact with the lumen; and a ring-like peripheral rim of
higher CT attenuation surrounding this central area (arrows); (C) Positive
remodeling, defined as the ratio of outer vessel diameter at the site of
plaque divided by the average outer diameter of the proximal and distal
vessel greater than 1.1, or Av/[(Ap + Ad)/2] >1.1; and (D) Low
attenuation plaque, defined as non-calcified plaque with internal
attenuation less than 30 HU. Please note that a combination of two or more
high-risk features is necessary to designate the plaque as high-risk for
CAD-RADS.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/ae9d/9627235/c0ab3a069aab/ryct.220183.fig15.jpg)
References
-
- Cury RC.. President's page: ten years of innovation in cardiac CT. J Cardiovasc Comput Tomogr. 2014 Jul-Aug;8(4):338–339. - PubMed
-
- Abbara S, Arbab-Zadeh A, Callister TQ, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009 May-Jun;3(3):190–204. - PubMed
-
- Leipsic J, Abbara S, Achenbach S, et al. SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2014 Sep-Oct;8(5):342–358. - PubMed
-
- Taylor AJ , Cerqueira M , Hodgson JM , et al . ACCF/SCCT/ACR/AHA/ASE/ASNC/ NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of cardiology foundation appropriate use criteria task force, the society of cardiovascular computed tomography, the American College of radiology, the American heart association, the American society of echocardiography, the American society of nuclear cardiology, the north American society for cardiovascular imaging, the society for cardiovascular angiography and interventions, and the society for cardiovascular magnetic resonance . J Cardiovasc Comput Tomogr . 2010. Nov-Dec ; 4 ( 6 ): 407.e1, 33 . - PubMed
-
- White RD , Patel MR , Abbara S , et al . American College of Radiology; American College of Cardiology Foundation. ACCF/ACR/ASE/ASNC/SCCT/SCMR appropriate utilization of cardiovascular imaging in heart failure: an executive summary: a joint report of the ACR Appropriateness Criteria ® Committee and the ACCF Appropriate Use Criteria Task Force . J Am Coll Radiol . 2013. ; 10 ( 7 ): 493 – 500 . - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
