

Homogeneous ensemble models for predicting infection levels and mortality of COVID-19 patients: Evidence from China
- PMID: 36339905
- PMCID: PMC9630904
- DOI: 10.1177/20552076221133692
Homogeneous ensemble models for predicting infection levels and mortality of COVID-19 patients: Evidence from China
Abstract
Background: Persistence of long-term COVID-19 pandemic is putting high pressure on healthcare services worldwide for several years. This article aims to establish models to predict infection levels and mortality of COVID-19 patients in China.
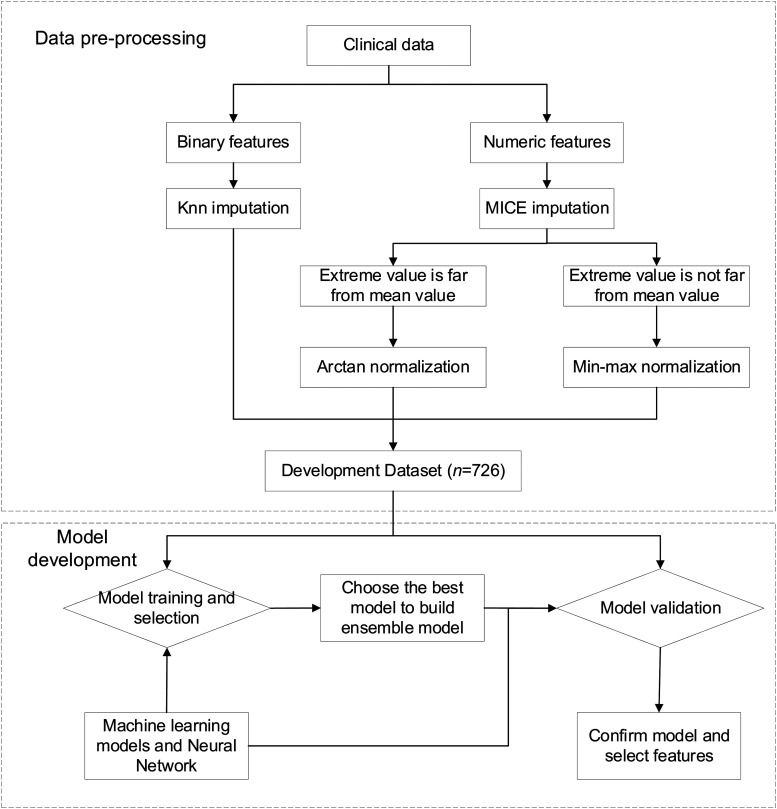
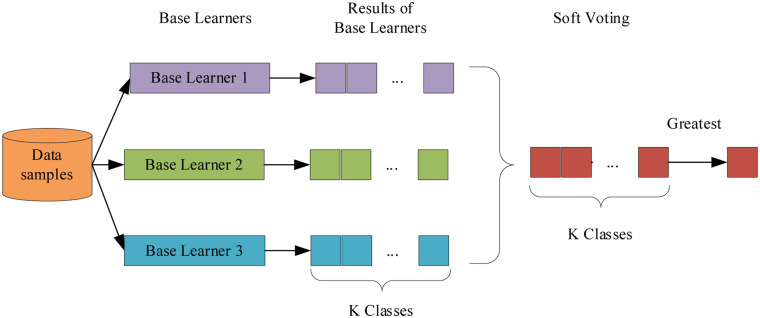
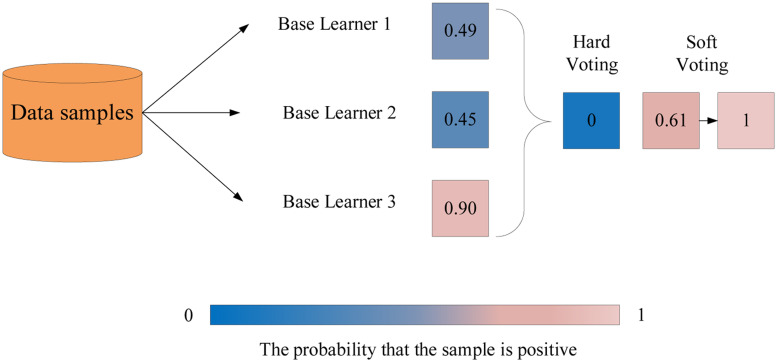
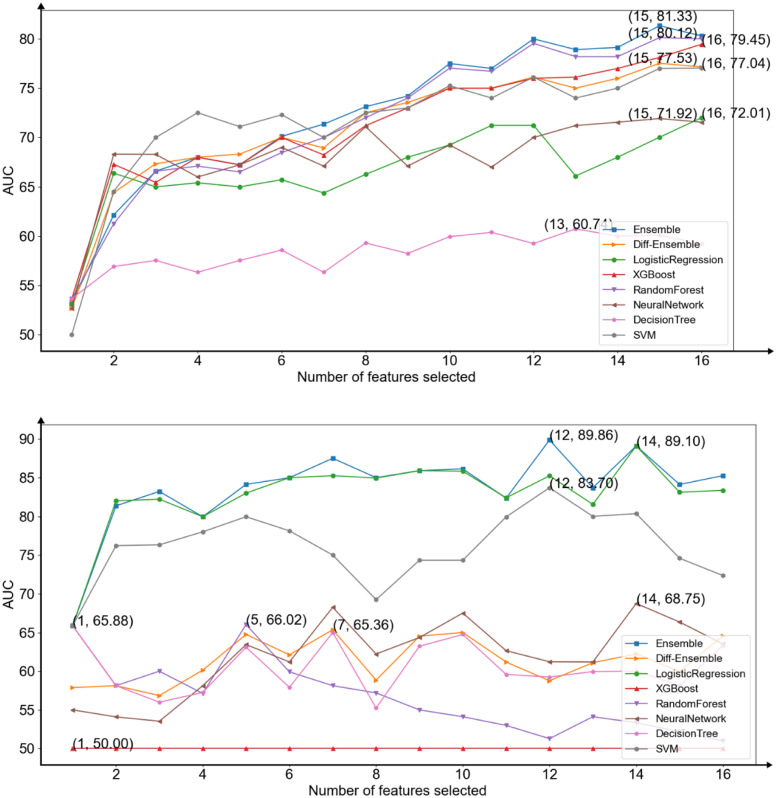
Methods: Machine learning models and deep learning models have been built based on the clinical features of COVID-19 patients. The best models are selected by area under the receiver operating characteristic curve (AUC) scores to construct two homogeneous ensemble models for predicting infection levels and mortality, respectively. The first-hand clinical data of 760 patients are collected from Zhongnan Hospital of Wuhan University between 3 January and 8 March 2020. We preprocess data with cleaning, imputation, and normalization.
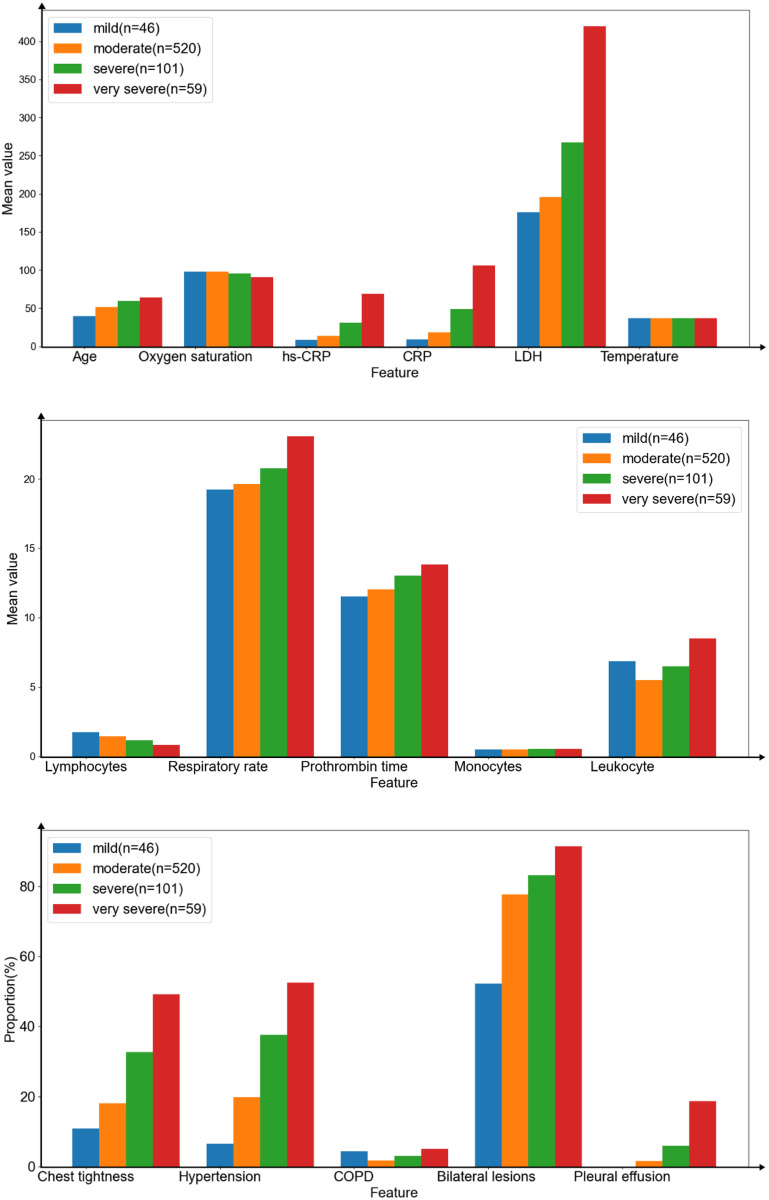
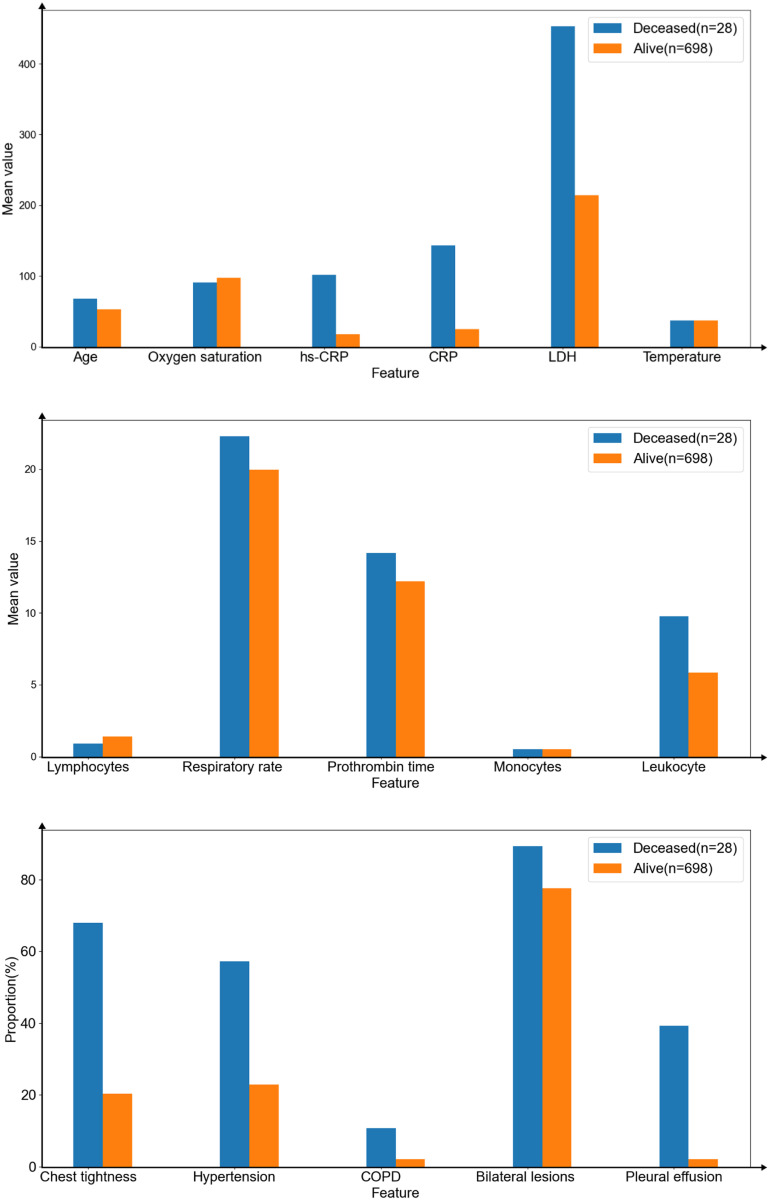
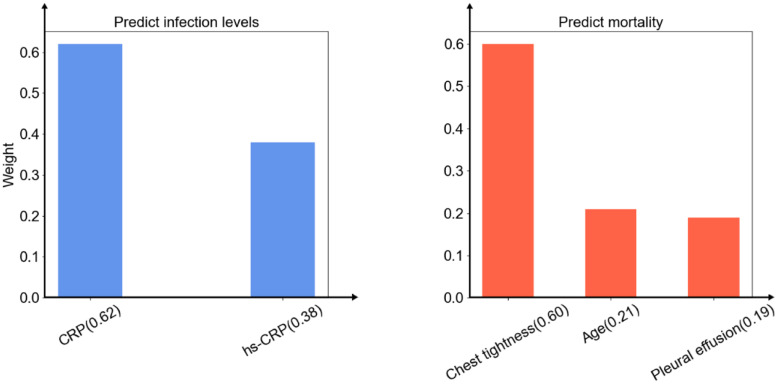
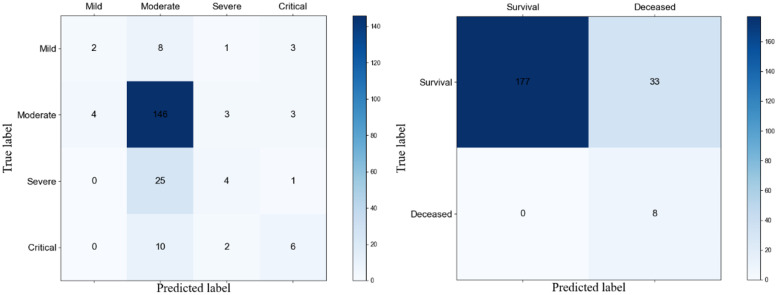
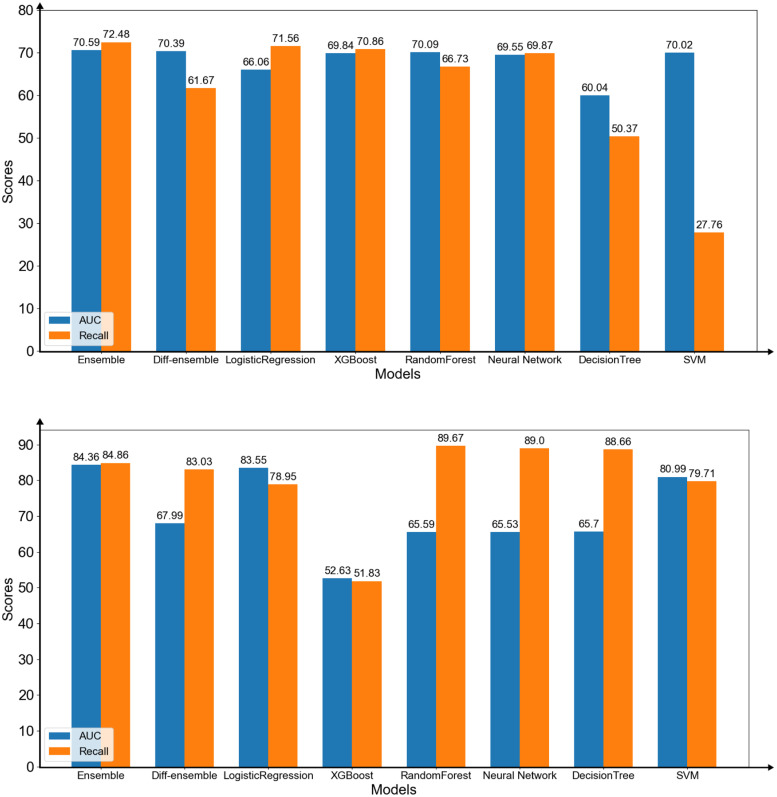
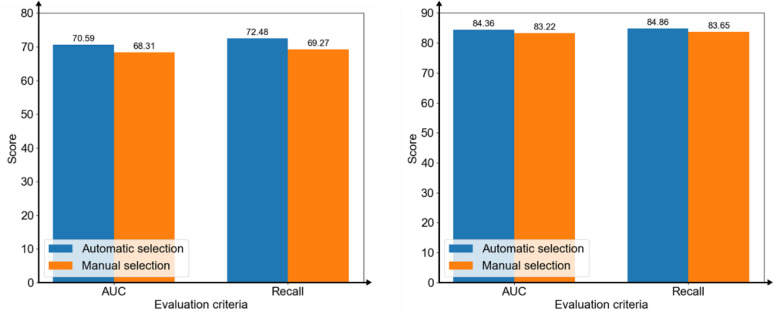
Results: Our models obtain AUC = 0.7059 and Recall (Weighted avg) = 0.7248 in predicting infection level, while AUC=0.8436 and Recall (Weighted avg) = 0.8486 in predicting mortality ratio. This study also identifies two sets of essential clinical features. One is C-reactive protein (CRP) or high sensitivity C-reactive protein (hs-CRP) and the other is chest tightness, age, and pleural effusion.
Conclusions: Two homogeneous ensemble models are proposed to predict infection levels and mortality of COVID-19 patients in China. New findings of clinical features for benefiting the machine learning models are reported. The evaluation of an actual dataset collected from January 3 to March 8, 2020 demonstrates the effectiveness of the models by comparing them with state-of-the-art models in prediction.
Keywords: COVID-19; Ensemble model; electronic health records; machine learning; prediction models.
© The Author(s) 2022.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- World Health Organization. COVID-19 weekly epidemiological update, edition 84, 22 March 2022. 2022.
-
- World Health Organization (WHO). Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected: interim guidance; WHO: Geneva, Switzerland; Available online: https://apps.who.int/iris/handle/10665/332299. Published 12 January 2020.
-
- Yan L, Zhang HT, Goncalves Jet al. An interpretable mortality prediction model for COVID-19 patients. Nat Mach Intell 2020; 2: 283–288.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
