

Lesion Index-guided workflow for the treatment of paroxysmal atrial fibrillation is safe and effective - Final results from the LSI Workflow Study
- PMID: 36340486
- PMCID: PMC9626745
- DOI: 10.1016/j.hroo.2022.06.004
Lesion Index-guided workflow for the treatment of paroxysmal atrial fibrillation is safe and effective - Final results from the LSI Workflow Study
Abstract
Background: Pulmonary vein isolation (PVI) ablation is a standard therapy for paroxysmal atrial fibrillation (PAF). Lesion Index (LSI) is a metric to guide radiofrequency (RF) ablation using the TactiCath Ablation Catheter, Sensor Enabled with the EnSite Cardiac Mapping System (Abbott).
Objective: This study (NCT-03906461) was designed to capture best practices using LSI-guided catheter ablation to treat PAF subjects in a real-world setting.
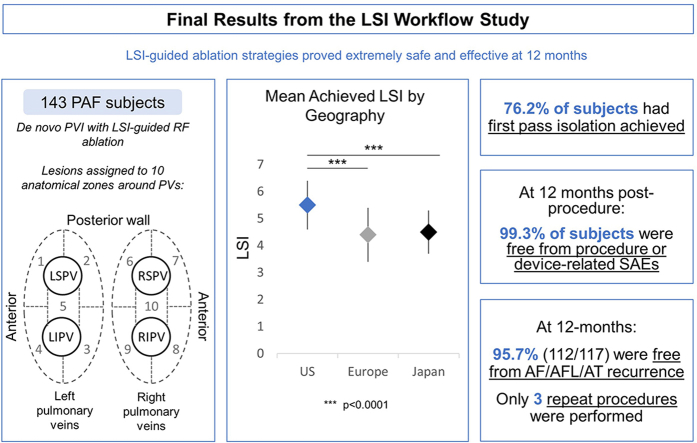
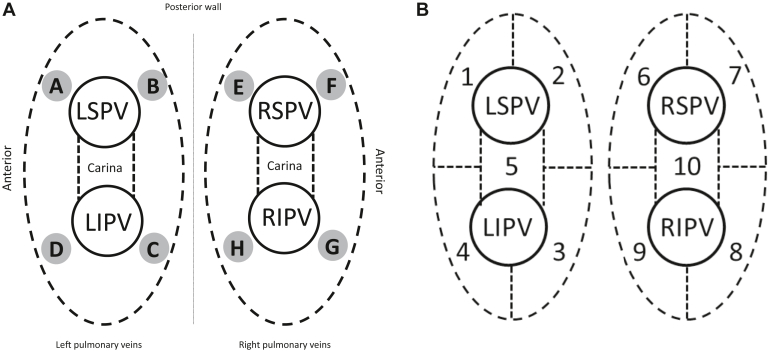
Methods: This prospective single-arm observational study enrolled 143 PAF subjects in the United States, Europe, and Japan undergoing de novo PVI with RF ablation. PVI lesions were assigned to 10 anatomically defined segments. Mean LSIs achieved for all lesions were analyzed. Follow-up was conducted between 3-6 months and 12 months after the procedure.
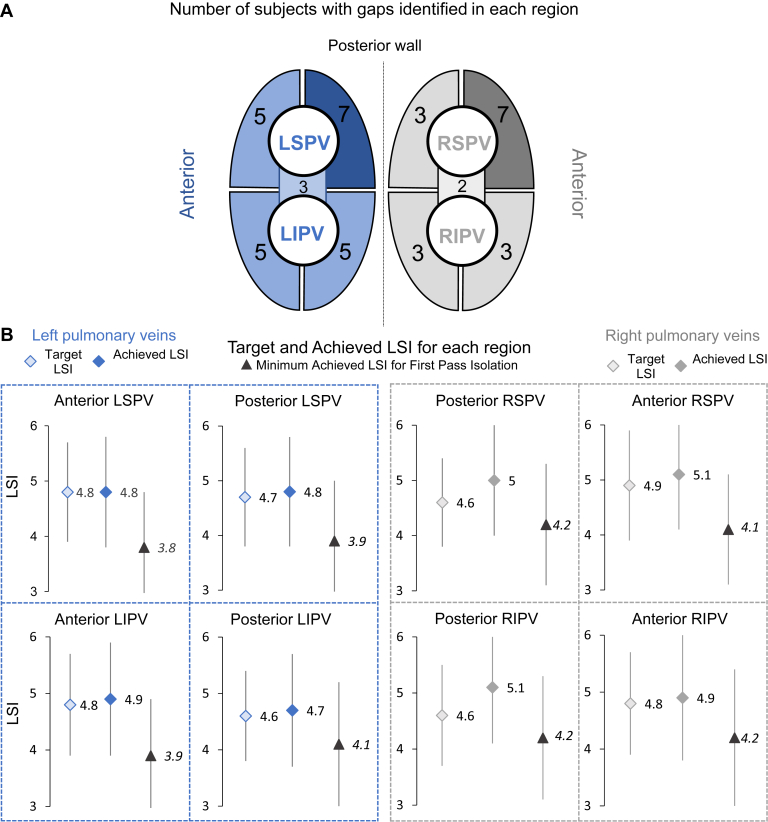
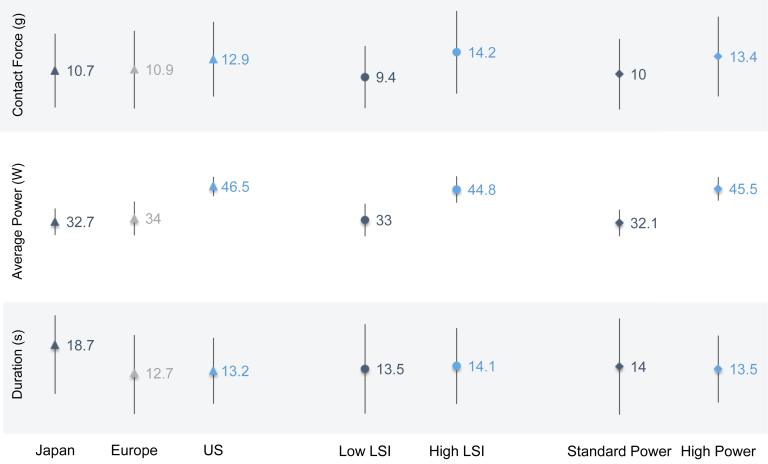
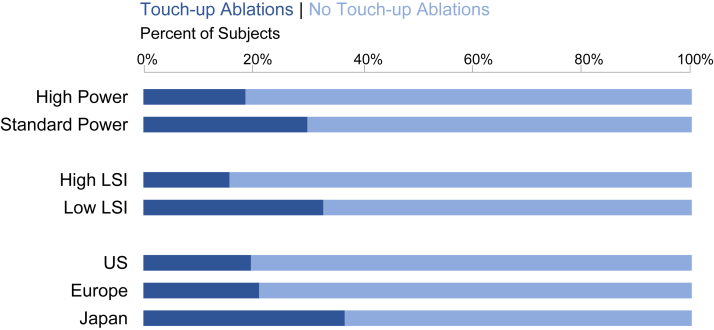
Results: Pulmonary veins were isolated in all subjects. The mean achieved LSI was 4.9, with lower values in Europe (4.4) and Japan (4.5) than the United States (5.5). First-pass success, defined as no gaps requiring touch-up ablation after 20 minutes post isolation, was achieved in 76.2% of subjects. Use of high LSI (≥5) resulted in shorter procedure, RF, and fluoroscopy times and fewer touch-up ablations compared to low LSI (<5). At 12 months, 99.3% of subjects were free from procedure- or device-related serious adverse events and 95.7% (112/117) (35.0% on antiarrhythmic drugs) were free from recurrence and/or a repeat ablation procedure for atrial fibrillation / atrial flutter / atrial tachycardia.
Conclusion: LSI-guided ablation strategies proved safe and effective despite differences in LSI workflows. Use of high LSI values resulted in shorter procedure, RF, and fluoroscopy times and fewer touch-up ablations compared to low LSI.
Keywords: Atrial fibrillation; Contact force; Lesion Index; Pulmonary vein isolation; Radiofrequency catheter ablation.
© 2022 Heart Rhythm Society. Published by Elsevier Inc.
Figures
References
-
- Kuck K.H., Reddy V.Y., Schmidt B., et al. A novel radiofrequency ablation catheter using contact force sensing: Toccata study. Heart Rhythm. 2012;9:18–23. - PubMed
-
- Neuzil P., Reddy V.Y., Kautzner J., et al. Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I study. Circ Arrhythm Electrophysiol. 2013;6:327–333. - PubMed
-
- Reddy V.Y., Shah D., Kautzner J., et al. The relationship between contact force and clinical outcome during radiofrequency catheter ablation of atrial fibrillation in the TOCCATA study. Heart Rhythm. 2012;9:1789–1795. - PubMed
-
- Kautzner J., Natale A., Michaud G., et al. Segmental variability in lesion size is controlled using contact force during pulmonary venous isolation. EP Europace. 2013;15:ii56–ii78.
LinkOut - more resources
Full Text Sources
