

Comparison of the Therapeutic Effect of the Mini-Open Incision and Conventional Open Neurolysis of the Median Nerve for Carpal Tunnel Syndrome
- PMID: 36340966
- PMCID: PMC9616651
- DOI: 10.1155/2022/4082618
Comparison of the Therapeutic Effect of the Mini-Open Incision and Conventional Open Neurolysis of the Median Nerve for Carpal Tunnel Syndrome
Abstract
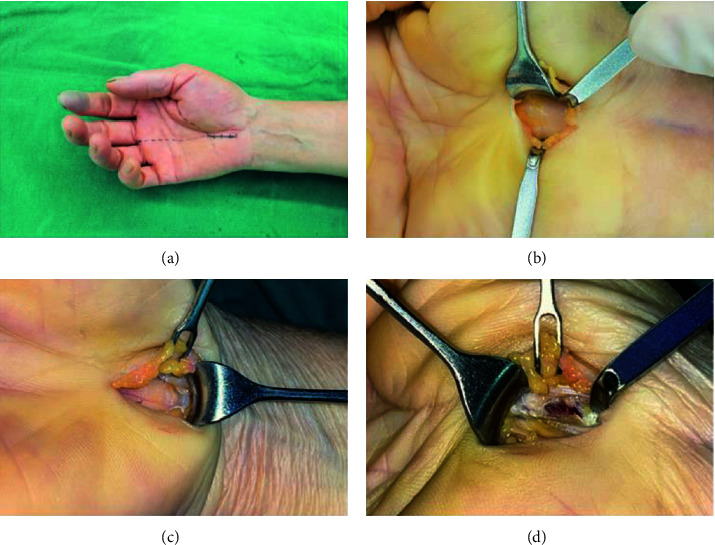
Objective: The aim of this study was to compare the therapeutic effects of the mini-open incision and conventional open surgery for carpal tunnel syndrome (CTS).
Methods: The clinical data of 52 patients with CTS treated at the First Affiliated Hospital of the University of Science and Technology of China from October 2020 to February 2022 were retrospectively analyzed. The patients were divided into the conventional open surgery group (28 cases) and the mini-open incision group (24 cases) according to different surgical incisions applied. The incision length, operation time, time until postoperative return to work, and complications were observed in the two groups. The Visual Analog Scale (VAS) for pain at one day, one month, and three months after surgery and the Boston Carpal Tunnel Questionnaire scores before, at one month, and at three months after surgery were compared between the two groups.
Results: The incision length, operation time, and time until return to work in the mini-open incision group were all shorter than those in the conventional open surgery group (2.58 ± 0.35 vs. 7.32 ± 0.61 cm, 18.67 ± 2.62 vs. 29.46 ± 3.42 min, and 5.33 ± 1.40 vs. 13.86 ± 2.70 d, respectively), and differences were statistically significant (P < 0.05 in all). The VAS scores in the mini-open incision group were lower than those in the conventional open surgery group at one day and one month after surgery, while the difference in the VAS scores at three months after surgery was not statistically significant between the two groups. There was no statistically significant difference in neurological recovery between the two groups at postoperative follow-ups (P > 0.05). The incidences of postoperative scar hyperplasia and scar pain were higher in the conventional open surgery group than those in the mini-open incision group, and differences were statistically significant (P < 0.05 in both).
Conclusion: Mini-open incision surgery for CTS was a safe and reliable procedure with a precise therapeutic effect, minimal surgical trauma, and high postoperative comfort for patients and could achieve enhanced recovery. Trial Registration. This trial is registered with ChiCTR2200064631.
Copyright © 2022 Feng Hu et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
Comparative Analysis of a New Device-Assisted Mini-Incision Versus Conventional Surgery for Carpal Tunnel Syndrome: A Retrospective Study of 109 Cases.Ther Clin Risk Manag. 2025 Apr 23;21:511-522. doi: 10.2147/TCRM.S514225. eCollection 2025. Ther Clin Risk Manag. 2025. PMID: 40290858 Free PMC article.
-
Comparing open conventional carpal tunnel release with mini-incision technique in the treatment of carpal tunnel syndrome: A non-randomized clinical trial.Ann Med Surg (Lond). 2020 May 16;55:119-123. doi: 10.1016/j.amsu.2020.05.001. eCollection 2020 Jul. Ann Med Surg (Lond). 2020. PMID: 32477509 Free PMC article.
-
Comparison of Wrist Arthroscopy, Small Incision Surgery, and Conventional Surgery for the Treatment of Carpal Tunnel Syndrome: A Retrospective Study at a Single Center.Med Sci Monit. 2019 Jun 3;25:4122-4129. doi: 10.12659/MSM.912912. Med Sci Monit. 2019. PMID: 31155608 Free PMC article.
-
Open median nerve release using double mini skin incision in patients with carpal tunnel syndrome: technique and clinical results.Neurol Med Chir (Tokyo). 2003 Sep;43(9):465-7; discussion 468. doi: 10.2176/nmc.43.465. Neurol Med Chir (Tokyo). 2003. PMID: 14560854 Review.
-
Carpal tunnel release via limited palmar incision.Hand Clin. 2002 May;18(2):299-306. doi: 10.1016/s0749-0712(01)00008-7. Hand Clin. 2002. PMID: 12371032 Review.
Cited by
-
Comprehensive analysis of knee cysts: diagnosis and treatment.Knee Surg Relat Res. 2025 May 14;37(1):23. doi: 10.1186/s43019-025-00269-2. Knee Surg Relat Res. 2025. PMID: 40369692 Free PMC article. Review.
-
Time to recovery following open and endoscopic carpal tunnel decompression: meta-analysis.BJS Open. 2025 Jul 1;9(4):zraf085. doi: 10.1093/bjsopen/zraf085. BJS Open. 2025. PMID: 40699057 Free PMC article.
-
Surgical Interventions for the Management of Carpal Tunnel Syndrome: A Narrative Review.Cureus. 2024 Mar 5;16(3):e55593. doi: 10.7759/cureus.55593. eCollection 2024 Mar. Cureus. 2024. PMID: 38576667 Free PMC article. Review.
-
Comparison of carpal tunnel release with double mini-incision approach and traditional approach: A retrospective study.Medicine (Baltimore). 2025 May 16;104(20):e42510. doi: 10.1097/MD.0000000000042510. Medicine (Baltimore). 2025. PMID: 40388748 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials