

Can cochlear implantation prevent cognitive decline in the long-term follow-up?
- PMID: 36341108
- PMCID: PMC9631779
- DOI: 10.3389/fneur.2022.1009087
Can cochlear implantation prevent cognitive decline in the long-term follow-up?
Abstract
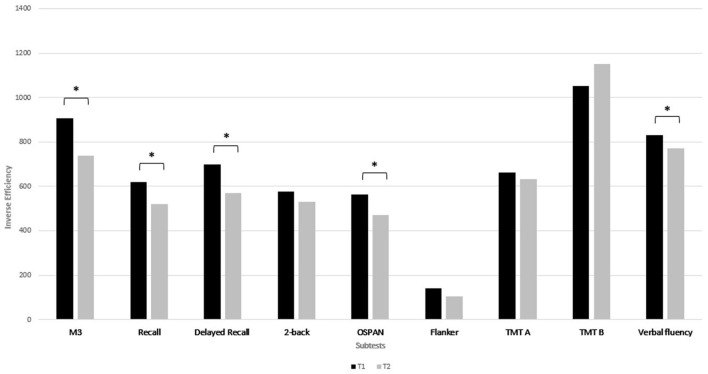
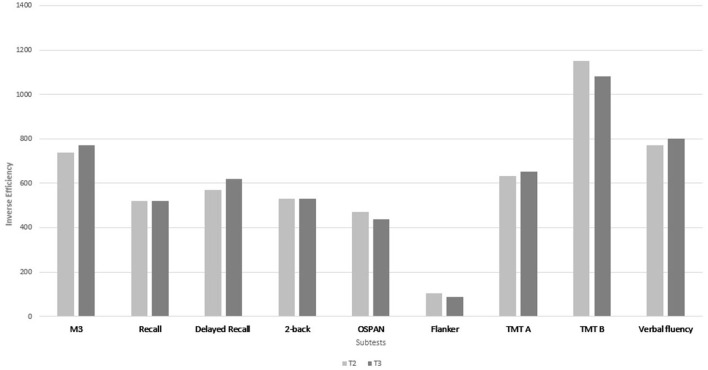
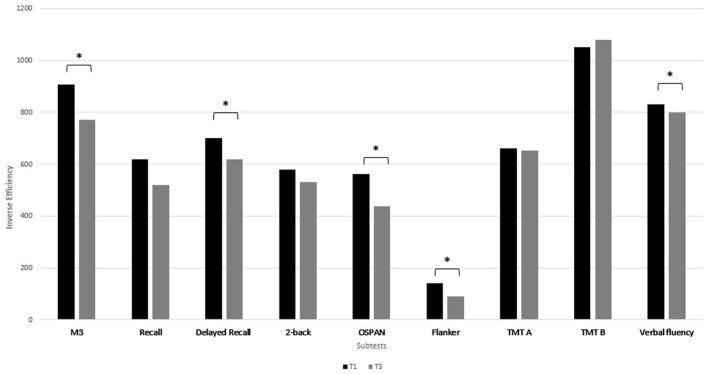
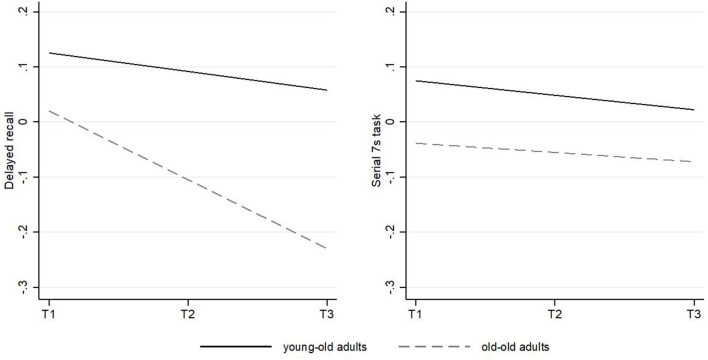
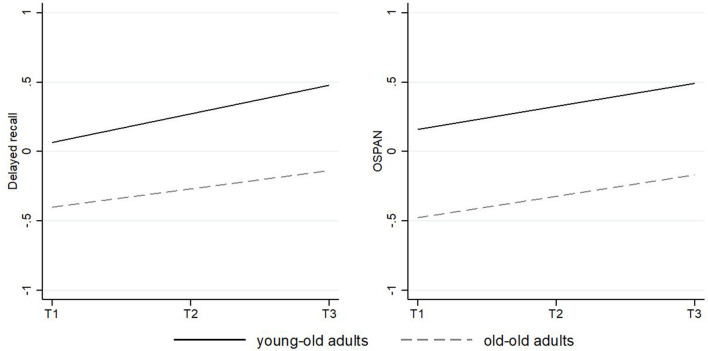
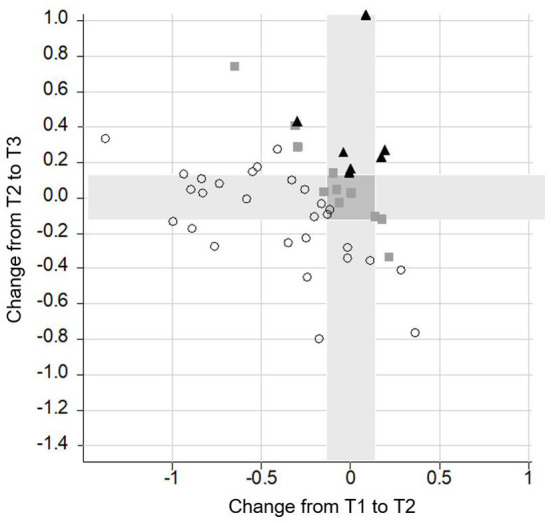
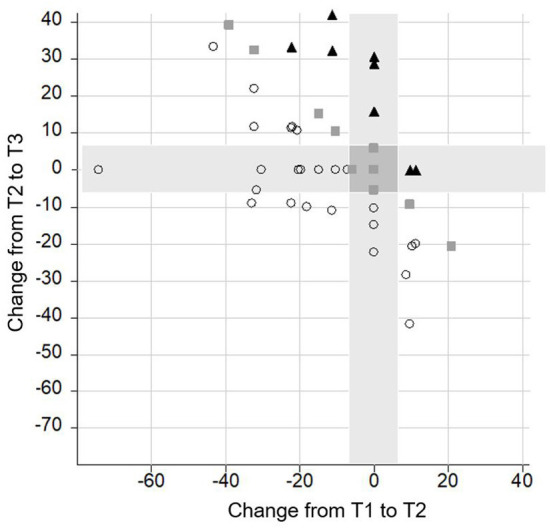
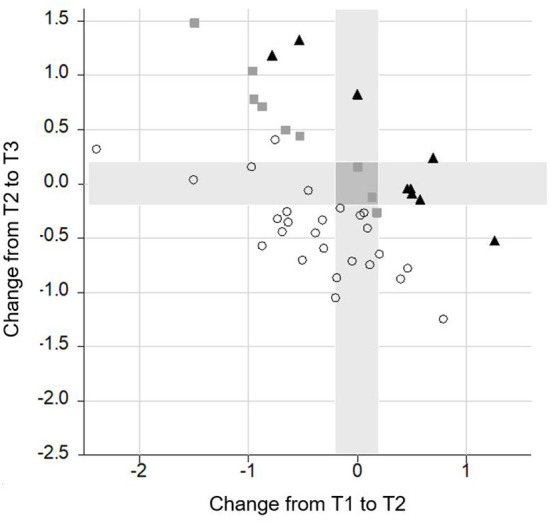
Cognitive function and hearing are known to both decline in older adults. As hearing loss is proposed to be one modifiable risk factor for dementia, the impact of auditory rehabilitation on cognitive decline has been gaining increasing attention. Despite a large number of studies, long-term data are still rare. In a large prospective longitudinal monocentric study, 50 adults (aged ≥ 50 years) with severe postlingual bilateral hearing loss received a cochlear implant (CI). They underwent comprehensive neurocognitive testing prior to implantation (T1), at 12 months (T2) and up to 65 months (T3) after implantation. Various cognitive subdomains such as attention, inhibition, working memory, verbal fluency, mental flexibility and (delayed) recall were assessed by the computer-based non-auditory test battery ALAcog©. The observed trajectories of two exemplary cognitive subdomains (delayed recall and working memory) were then fitted over time using multilevel growth models to adjust for sociodemographic covariates and compared with 5-year longitudinal data from a sample of older adults from the representative Survey of Health, Aging and Retirement in Europe (SHARE) study. Postoperatively, auditory functions improved from 6.98% (SD 12.83) to 57.29% (SD 20.18) in monosyllabic speech understanding. Cognitive functions significantly increased from T1 to T3 in attention (p = 0.001), delayed recall (p = 0.001), working memory (OSPAN; p = 0.001), verbal fluency (p = 0.004), and inhibition (p = 0.002). A closer look at follow-up revealed that cognitive improvement could be detected between T1 and T2 and thereafter remained stable in all subtests (p ≥ 0.06). Additional longitudinal analysis confirmed these findings in a rigorous multilevel approach in two exemplary cognitive subdomains. In contrast to the SHARE data, there was no evidence for age-differential associations over time in CI recipients. This suggests that older adults benefit equally from cochlear implantation. CI users with worse preoperative cognitive skills experienced the most benefit (p < 0.0001). Auditory rehabilitation by cochlear implantation has a stimulating effect on cognitive functions beyond an improvement in speech understanding and an increased well-being. Large multicenter studies using standardized protocols have to be undertaken in the future to find out whether hearing restoration might help to prevent cognitive decline.
Keywords: auditory rehabilitation; cochlear implant; dementia; hearing loss; prevention.
Copyright © 2022 Völter, Götze, Kamin, Haubitz, Dazert and Thomas.
Conflict of interest statement
Authors CV, JT, and SD have received reimbursement of scientific meeting participation fees and accommodation expenses, as well as honoraria for preparing continuing medical education events and funding for research projects that they initiated, from MED-EL. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- WHO. World FAILING to Address Dementia Challenge. (2021). Available online at: https://www.who.int/news/item/02-09-2021-world-failing-to-address-dement... (accessed July 19, 2022).
LinkOut - more resources
Full Text Sources
Research Materials