

Clinical characteristics of combined rosacea and migraine
- PMID: 36341245
- PMCID: PMC9635264
- DOI: 10.3389/fmed.2022.1026447
Clinical characteristics of combined rosacea and migraine
Abstract
Background: An overlap between the skin disease rosacea and the headache disease migraine has been established; however, the magnitude of this overlap and the distribution between subtypes/phenotypes remains unclear.
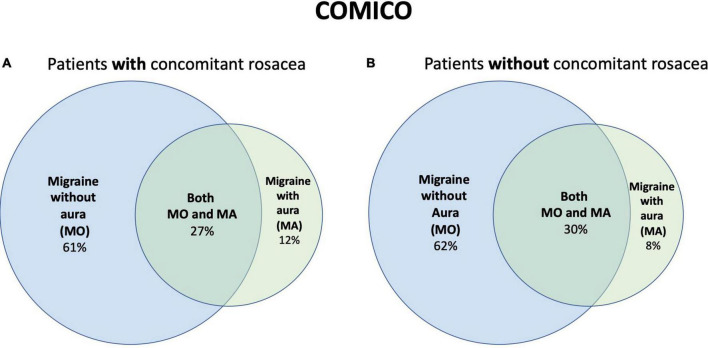
Objective: The aim was to determine the magnitude of the overlap between rosacea and migraine, and to determine which subtypes/phenotypes were present in patients with concomitant rosacea and migraine.
Methods: In this cross-sectional study, 604 patients with a diagnosis of either rosacea or migraine were phenotyped through a face-to-face interview with clinical examination, to determine prevalence and phenotype of rosacea, and prevalence and subtype of migraine.
Results: We found a prevalence of migraine of 54% in patients with rosacea, and a prevalence of rosacea of 65% in patients with migraine. Concomitant migraine was significantly associated with the rosacea features flushing (odds ratio = 2.6, 95% confidence interval = 1.4-4.7, p = 0.002), ocular symptoms (odds ratio = 2.4, 95% confidence interval = 1.5-3.9, p < 0.001), and burning (odds ratio = 2.1, 95% confidence interval = 1.3-3.4, p = 0.002), whereas papules/pustules were inversely related with concomitant migraine (odds ratio = 0.5, 95% confidence interval = 0.3-0.8, p = 0.006). No association was found between concomitant migraine and centrofacial erythema, rhinophyma, telangiectasia, edema, or dryness. Concomitant rosacea was not associated with any specific migraine subtype in patients with migraine.
Conclusion: This study highlights a substantial overlap between rosacea and migraine, particularly in patients with certain rosacea features. Individuals with rosacea should be asked about concomitant migraine, and comorbidities should be considered when choosing between treatments.
Keywords: interview; migraine; overlap; prevalence; rosacea.
Copyright © 2022 Wienholtz, Christensen, Zhang, Rechnagel, Byrnel, Haugaard, Ashina, Thyssen and Egeberg.
Conflict of interest statement
NW has acted as an invited speaker for Novartis and received a travel grant from the Kgl Hofbundtmager Aage Bang Foundation. CC has received personal fees from Teva and serves as a consultant for Teva. MA has received consulting fees and advisory boards fees from Alder, Allergan, Amgen, Eli Lilly, Lundbeck, Novartis, and Teva; fees for serving as a principal investigator, paid to his institution, from Alder, Allergan, Amgen, Electro-Core, Eli Lilly, Lundbeck, Novartis, and Teva; and grant support, paid to his institution, from Novo Nordisk Foundation, Novartis, and Lundbeck Foundation. JT has been an advisor, investigator, and speaker for Abbvie, Pfizer, LEO Pharma, Sanofi-Genzyme, Eli Lilly & Co., and Regeneron. He has received grants from Sanofi-Genzyme and Regeneron. AE has received research funding from Pfizer, Eli Lilly, the Danish National Psoriasis Foundation, and the Kgl Hofbundtmager Aage Bang Foundation and honoraria as consultant and/or speaker from Almirall, Leo Pharma, Samsung Bioepis Co., Ltd. Pfizer, Eli Lilly & Co., Novartis, Galderma, Dermavant, Bristol-Myers Squibb, and Janssen Pharmaceuticals. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
The relationship between migraine and rosacea: Systematic review and meta-analysis.Cephalalgia. 2018 Jun;38(7):1387-1398. doi: 10.1177/0333102417731777. Epub 2017 Sep 18. Cephalalgia. 2018. PMID: 28920449
-
[Signs and symptoms of rosacea].Ann Dermatol Venereol. 2014 Sep;141 Suppl 2:S151-7. doi: 10.1016/S0151-9638(14)70152-8. Ann Dermatol Venereol. 2014. PMID: 25151930 French.
-
Pharmacologic treatments for rosacea.Clin Dermatol. 2017 Mar-Apr;35(2):207-212. doi: 10.1016/j.clindermatol.2016.10.016. Epub 2016 Oct 27. Clin Dermatol. 2017. PMID: 28274361
-
Rosacea.2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32491506 Free Books & Documents.
-
Dermatology: how to manage rosacea in skin of colour.Drugs Context. 2022 May 31;11:2021-11-1. doi: 10.7573/dic.2021-11-1. eCollection 2022. Drugs Context. 2022. PMID: 35720055 Free PMC article. Review.
Cited by
-
Evaluation of Dermatological and Neurological Aspects of the Relationship between Rosacea and Headaches.Diagnostics (Basel). 2023 Dec 22;14(1):23. doi: 10.3390/diagnostics14010023. Diagnostics (Basel). 2023. PMID: 38201332 Free PMC article.
References
-
- Stovner LJ, Nichols E, Steiner TJ, Abd-Allah F, Abdelalim A, Al-Raddadi RM, et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. (2018) 17:954–76. 10.1016/S1474-4422(18)30322-3 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources