

Practice patterns and adherence to society guidelines for suspected choledocholithiasis: A comparison of academic and community settings from a large US healthcare system
- PMID: 36341246
- PMCID: PMC9631824
- DOI: 10.3389/fmed.2022.1000368
Practice patterns and adherence to society guidelines for suspected choledocholithiasis: A comparison of academic and community settings from a large US healthcare system
Abstract
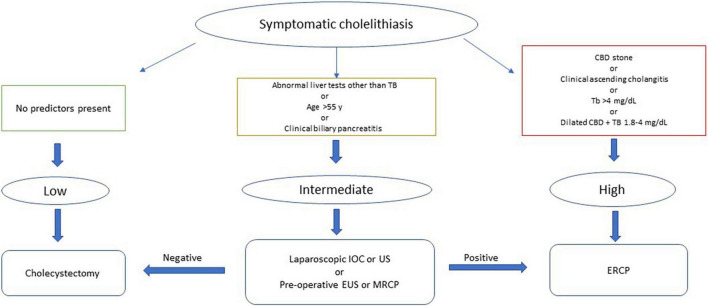
Background: The American Society of Gastrointestinal Endoscopy (ASGE) has proposed practice guidelines for evaluating patients with suspected choledocholithiasis. This study aims to assess and compare practice patterns for following ASGE guidelines for choledocholithiasis in a large academic vs. community hospital setting.
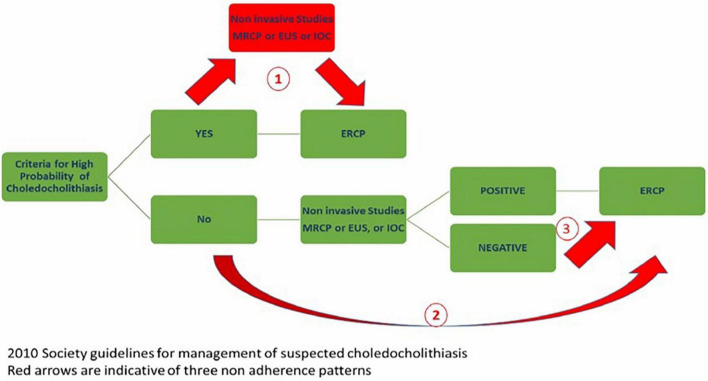
Methods: A total of one thousand ER indicated for choledocholithiasis were randomly selected. Patients' demographics, total bilirubin, imaging studies including magnetic resonance cholangiopancreatography (MRCP), intraoperative cholangiogram (IOC), endoscopic ultrasound (EUS), and ERCP results were retrospectively collected. Patients with prior sphincterotomy were excluded. We examined the following practice deviations from the current ASGE guidelines; (1) ERCP was potentially delayed in high probability cases while awaiting additional imaging studies, (2) ERCP was performed without additional imaging studies in cases of low/intermediate-risk, or (3) ERCP was performed in low/intermediate-risk cases when additional imaging studies were negative.
Results: A total of 640 patients with native papilla who underwent ERCP were included in the final analysis. Overall, the management of 43% (275) of patients was deviated from the applicable ASGE guidelines. Academic and community provider rates of non-adherence were 32 vs. 45%, respectively (p-value: < 0.01). Of 381 high-risk cases, 54.1% had additional imaging before ERCP. (Academic vs. community; 11.7 vs. 88.3%, p-value: < 0.01). In 26.7% (69/258) of low/intermediate risk cases, ERCP was performed without additional studies; academic (14.5%) vs. community (85.5%) (p-value: < 0.01). Finally, in 11.2% (19/170) of patients, ERCP was performed despite intermediate/low probability and negative imaging; academic (26.3%) vs. community (73.7%) (p-value: 0.02).
Conclusion: Our study results show that providers do not adhere to ASGE practice guidelines in 43% of suspected choledocholithiasis cases. The rate of non-adherence was significantly higher in community settings. It could be due to various reasons, including lack/delays for alternate studies (i.e., MRCP, EUS), concern regarding the length of stay, patient preference, or lack of awareness/understanding of the guidelines. Increased availability of alternate imaging and educational strategies may be needed to increase the adoption of practice guidelines across academic and community settings to improve patient outcomes and save healthcare dollars.
Keywords: American Society of Gastrointestinal Endoscopy (ASGE); adherence; choledocholithiasis; endoscopic retrograde cholangiopancreatography (ERCP); practice guidelines.
Copyright © 2022 Rashtak, Goyal, Chandran, Dedania, Patil, Wadhwa, Guha, Davee, Ramireddy and Thosani.
Conflict of interest statement
NT was a consultant for Boston-Scientific, Medtronic, Pentax America, received royalty from UpToDate, and was a speaker for Abbvie. SG was a consultant for Medtronic. HG was a consultant for Aimloxy LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Evaluating the accuracy of American Society for Gastrointestinal Endoscopy guidelines in patients with acute gallstone pancreatitis with choledocholithiasis.World J Gastroenterol. 2022 Apr 28;28(16):1692-1704. doi: 10.3748/wjg.v28.i16.1692. World J Gastroenterol. 2022. PMID: 35581962 Free PMC article.
-
Comparing diagnostic accuracy of current practice guidelines in predicting choledocholithiasis: outcomes from a large healthcare system comprising both academic and community settings.Gastrointest Endosc. 2021 Jun;93(6):1351-1359. doi: 10.1016/j.gie.2020.10.033. Epub 2020 Nov 5. Gastrointest Endosc. 2021. PMID: 33160977
-
Accuracy of ASGE high-risk criteria in evaluation of patients with suspected common bile duct stones.Gastrointest Endosc. 2017 Sep;86(3):525-532. doi: 10.1016/j.gie.2017.01.039. Epub 2017 Feb 4. Gastrointest Endosc. 2017. PMID: 28174126
-
Utility of MRCP in clinical decision making of suspected choledocholithiasis: An institutional analysis and literature review.Am J Surg. 2017 Aug;214(2):251-255. doi: 10.1016/j.amjsurg.2016.10.025. Epub 2016 Dec 1. Am J Surg. 2017. PMID: 27986260 Review.
-
Management of suspected common bile duct stones in children: role of selective intraoperative cholangiogram and endoscopic retrograde cholangiopancreatography.J Pediatr Surg. 2004 Jun;39(6):808-12; discussion 808-12. doi: 10.1016/j.jpedsurg.2004.02.019. J Pediatr Surg. 2004. PMID: 15185201 Review.
Cited by
-
Molecular Tumor Testing on Colorectal Adenocarcinoma Specimens in a Large Community-Based Healthcare System.J Patient Cent Res Rev. 2024 Oct 15;11(3):215-221. doi: 10.17294/2330-0698.2074. eCollection 2024 Fall. J Patient Cent Res Rev. 2024. PMID: 39439537 Free PMC article.
References
LinkOut - more resources
Full Text Sources