

Age-stratified infection fatality rate of COVID-19 in the non-elderly population
- PMID: 36341800
- PMCID: PMC9613797
- DOI: 10.1016/j.envres.2022.114655
Age-stratified infection fatality rate of COVID-19 in the non-elderly population
Abstract
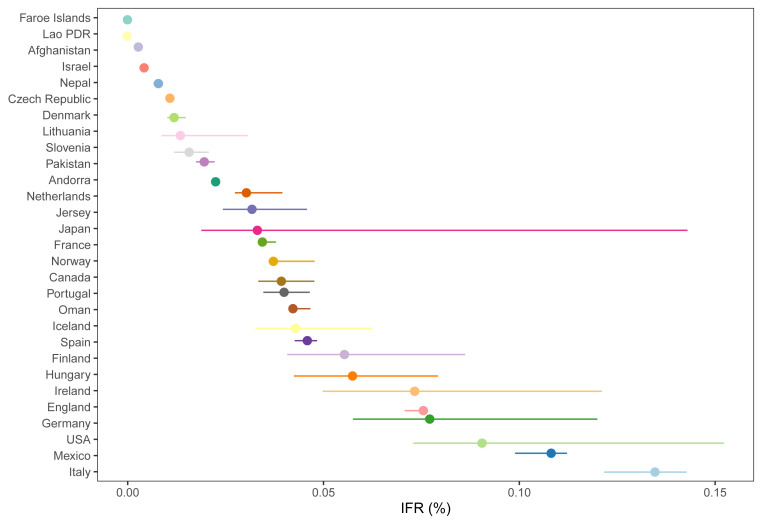
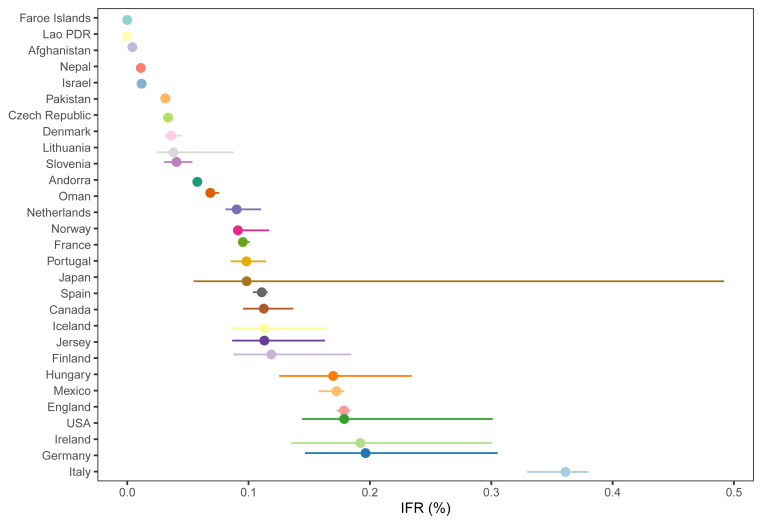
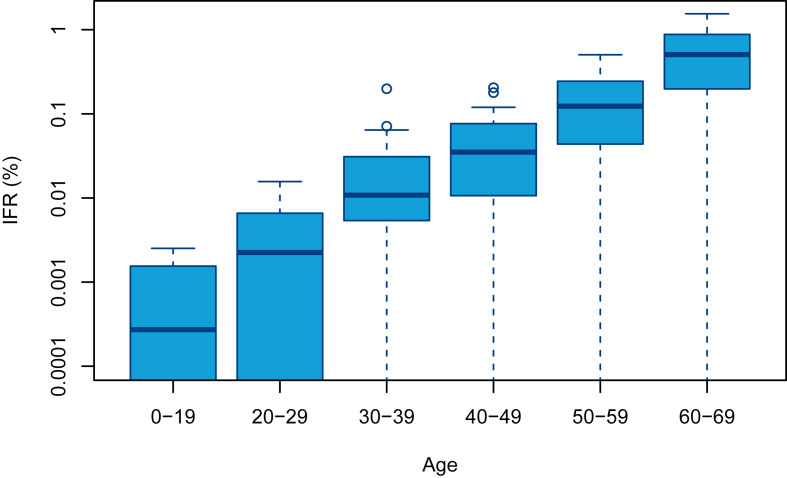
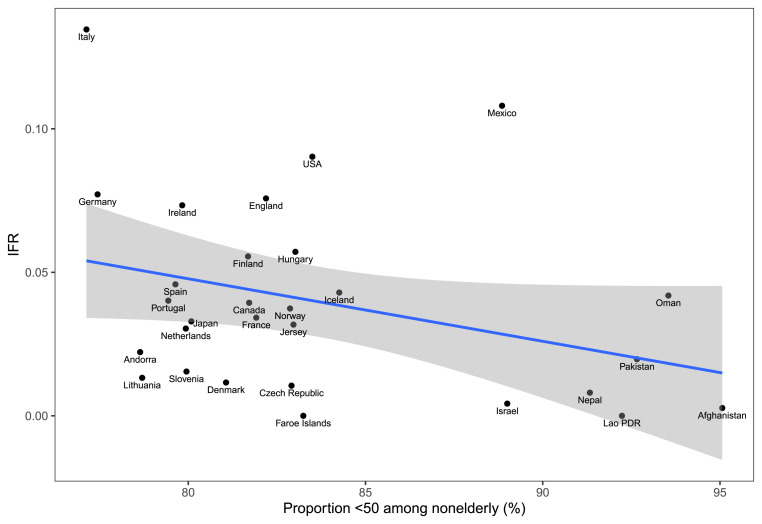
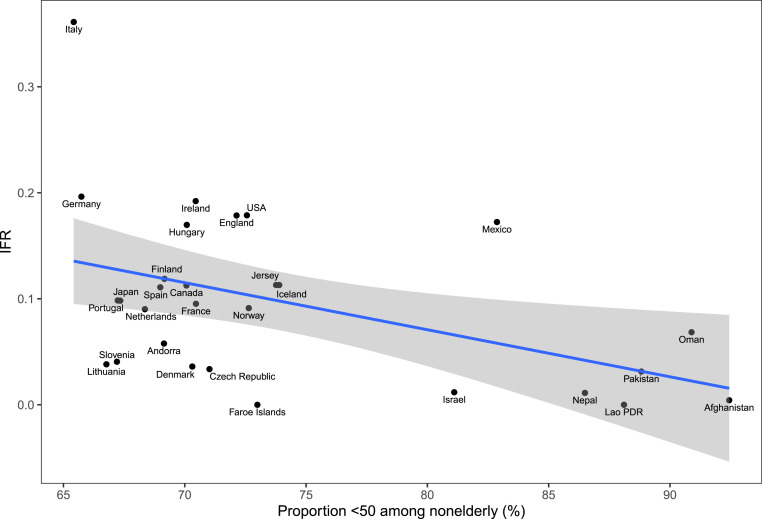
The largest burden of COVID-19 is carried by the elderly, and persons living in nursing homes are particularly vulnerable. However, 94% of the global population is younger than 70 years and 86% is younger than 60 years. The objective of this study was to accurately estimate the infection fatality rate (IFR) of COVID-19 among non-elderly people in the absence of vaccination or prior infection. In systematic searches in SeroTracker and PubMed (protocol: https://osf.io/xvupr), we identified 40 eligible national seroprevalence studies covering 38 countries with pre-vaccination seroprevalence data. For 29 countries (24 high-income, 5 others), publicly available age-stratified COVID-19 death data and age-stratified seroprevalence information were available and were included in the primary analysis. The IFRs had a median of 0.034% (interquartile range (IQR) 0.013-0.056%) for the 0-59 years old population, and 0.095% (IQR 0.036-0.119%) for the 0-69 years old. The median IFR was 0.0003% at 0-19 years, 0.002% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.123% at 50-59 years, and 0.506% at 60-69 years. IFR increases approximately 4 times every 10 years. Including data from another 9 countries with imputed age distribution of COVID-19 deaths yielded median IFR of 0.025-0.032% for 0-59 years and 0.063-0.082% for 0-69 years. Meta-regression analyses also suggested global IFR of 0.03% and 0.07%, respectively in these age groups. The current analysis suggests a much lower pre-vaccination IFR in non-elderly populations than previously suggested. Large differences did exist between countries and may reflect differences in comorbidities and other factors. These estimates provide a baseline from which to fathom further IFR declines with the widespread use of vaccination, prior infections, and evolution of new variants.
Keywords: Bias; COVID-19; Epidemics; Infection fatality rate; Seroprevalence.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Adam D. The pandemic's true death toll: millions more than official counts. Nature. 2022;601(7893):312–315. Jan. - PubMed
-
- Agyemang C., et al. In: Metabolic Syndrome. Ahima R.S., editor. Springer International Publishing; Switzerland: 2016. Chapter 4. Obesity in sub-saharan Africa.https://link.springer.com/content/pdf/10.1007/978-3-319-11251-0_5.pdf - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
