

Changes in prenatal care and birth outcomes after federally qualified health center expansion
- PMID: 36342016
- PMCID: PMC10012219
- DOI: 10.1111/1475-6773.14099
Changes in prenatal care and birth outcomes after federally qualified health center expansion
Abstract
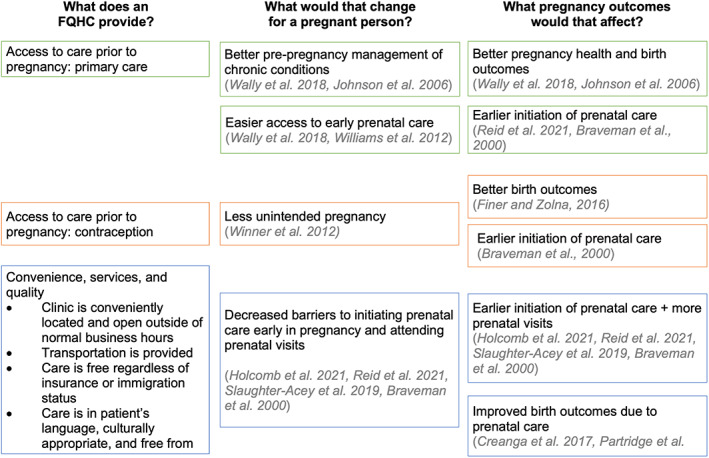
Objective: To evaluate whether the expansion of Federally Qualified Health Centers (FQHCs) improved late prenatal care initiation, low birth weight, and preterm birth among Medicaid-covered or uninsured individuals.
Data sources and study setting: We identified all FQHCs in California using the Health Resources and Services Administration's Uniform Data System from 2000 to 2019. We used data from the U.S. Census American Community Survey to describe area characteristics. We measured outcomes in California birth certificate data from 2007 to 2019.
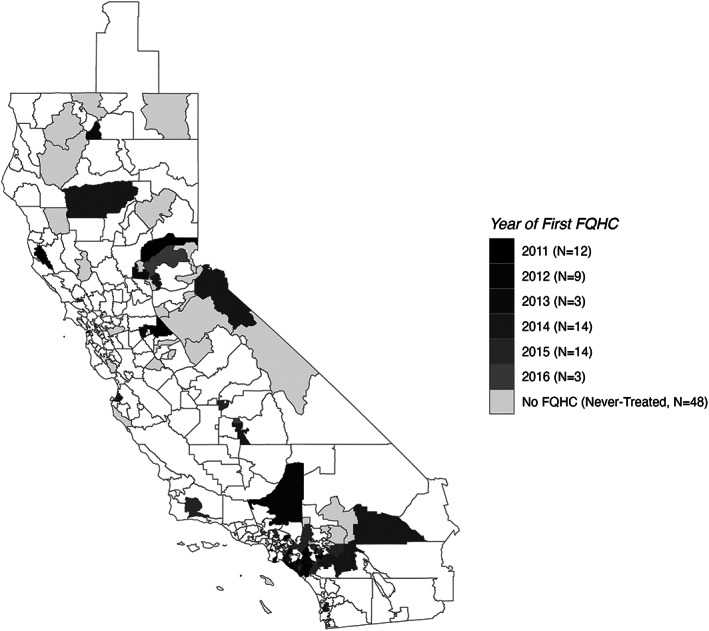
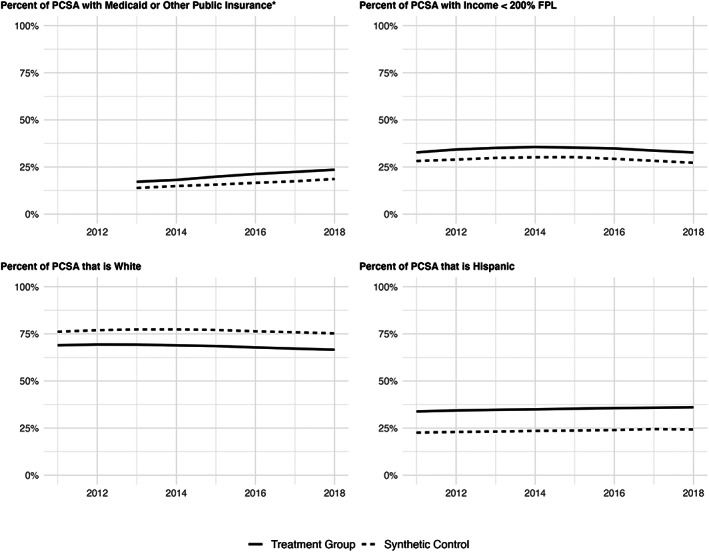
Study design: We compared areas that received their first FQHC between 2011 and 2016 to areas that received it later or that had never had an FQHC. Specifically, we used a synthetic control with a staggered adoption approach to calculate non-parametric estimates of the average treatment effects on the treated areas. The key outcome variables were the rate of Medicaid or uninsured births with late prenatal care initiation (>3 months' gestation), with low birth weight (<2500 grams), or with preterm birth (<37 weeks' gestation).
Data collection/extraction methods: The analysis was limited to births covered by Medicaid or that were uninsured, as indicated on the birth certificate.
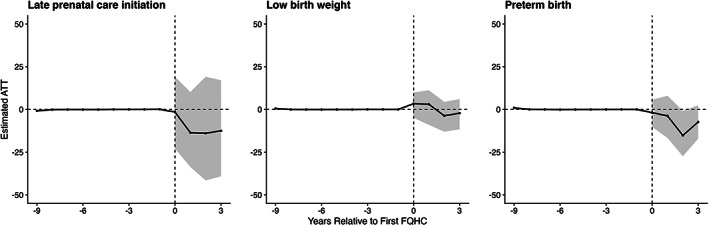
Principal findings: The 55 areas in California that received their first FQHC in 2011-2016 were more populous; their residents were more likely to be covered by Medicaid, to be low-income, or to be Hispanic than residents of the 48 areas that did not have an FQHC by the end of the study period. We found no statistically significant impact of the first FQHC on rates of late prenatal care initiation (ATT: -10.4 [95% CI -38.1, 15.0]), low birth weight (ATT: 0.2 [95% CI -7.1, 5.4]), or preterm birth (ATT: -7.0 [95% CI -15.5, 2.3]).
Conclusions: Our results from California suggest that access to primary and prenatal care may not be enough to improve these outcomes. Future work should evaluate the impact of ongoing initiatives to increase access to maternal health care at FQHCs through targeted workforce investments.
Keywords: Medicaid; maternal and perinatal care and outcomes; observational data/quasi-experiments; obstetrics/gynecology; uninsured/safety net providers.
© 2022 The Authors. Health Services Research published by Wiley Periodicals LLC on behalf of Health Research and Educational Trust.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Access to Federally Qualified Health Centers and Emergency Department Use Among Uninsured and Medicaid-insured Adults: California, 2005 to 2013.Acad Emerg Med. 2019 Feb;26(2):129-139. doi: 10.1111/acem.13494. Epub 2019 Jan 16. Acad Emerg Med. 2019. PMID: 30648780 Free PMC article.
-
Federally Qualified Health Center Access and Emergency Department Use Among Children.Pediatrics. 2016 Oct;138(4):e20160479. doi: 10.1542/peds.2016-0479. Pediatrics. 2016. PMID: 27660059
-
Estimating the Impact of Medicaid Expansion and Federal Funding Cuts on FQHC Staffing and Patient Capacity.Milbank Q. 2022 Jun;100(2):504-524. doi: 10.1111/1468-0009.12560. Epub 2022 Apr 12. Milbank Q. 2022. PMID: 35411969 Free PMC article.
-
Medicaid and preterm birth and low birth weight: the last two decades.J Womens Health (Larchmt). 2010 Mar;19(3):443-51. doi: 10.1089/jwh.2009.1602. J Womens Health (Larchmt). 2010. PMID: 20141370 Free PMC article. Review.
-
The ACA Medicaid Expansion And Perinatal Insurance, Health Care Use, And Health Outcomes: A Systematic Review.Health Aff (Millwood). 2022 Jan;41(1):60-68. doi: 10.1377/hlthaff.2021.01150. Health Aff (Millwood). 2022. PMID: 34982621
Cited by
-
Effects of information-knowledge-attitude-practice health education combined with cluster-based care in patients with gestational hypertension.Medicine (Baltimore). 2023 Oct 13;102(41):e35346. doi: 10.1097/MD.0000000000035346. Medicine (Baltimore). 2023. PMID: 37832047 Free PMC article. Clinical Trial.
-
Patient experiences with prenatal cell-free DNA screening in a safety net setting.Prenat Diagn. 2024 Apr;44(4):409-417. doi: 10.1002/pd.6541. Epub 2024 Feb 29. Prenat Diagn. 2024. PMID: 38423995 Free PMC article.
-
Low birthweight rate differences associated with distinct perinatal staffing mixes at federally funded health centers.Health Aff Sch. 2024 Dec 4;2(12):qxae113. doi: 10.1093/haschl/qxae113. eCollection 2024 Dec. Health Aff Sch. 2024. PMID: 39664479 Free PMC article.
References
-
- Tikkanen R, Gunja MZ, FitzGerald M, Zephyrin L. Maternal mortality and maternity Care in the United States Compared to 10 other developed countries. The Commonwealth Fund. 10.26099/411v-9255 - DOI
-
- MacDorman MF, Mathews TJ, Mohangoo AD, Zeitlin J. International comparisons of infant mortality and related factors: United States and Europe, 2010; 2014:7. - PubMed
-
- Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes . In: Behrman RE, Butler AS, eds. Preterm Birth: Causes, Consequences, and Prevention. National Academies Press (US); 2007. Accessed January 20, 2022. http://www.ncbi.nlm.nih.gov/books/NBK11362/ - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
