

SARS-CoV-2 Vaccine Immunogenicity in Patients with Gastrointestinal Cancer Receiving Systemic Anti-Cancer Therapy
- PMID: 36342104
- PMCID: PMC9847553
- DOI: 10.1093/oncolo/oyac230
SARS-CoV-2 Vaccine Immunogenicity in Patients with Gastrointestinal Cancer Receiving Systemic Anti-Cancer Therapy
Abstract
Introduction: Patients with gastrointestinal (GI) cancers have an increased risk of serious complications and death from SARS-CoV-2 infection. The immunogenicity of vaccines in patients with GI cancers receiving anti-cancer therapies is unclear. We conducted a prospective study to evaluate the prevalence of neutralizing antibodies in a cohort of GI cancer patients receiving chemotherapy following SARS-CoV-2 vaccination.
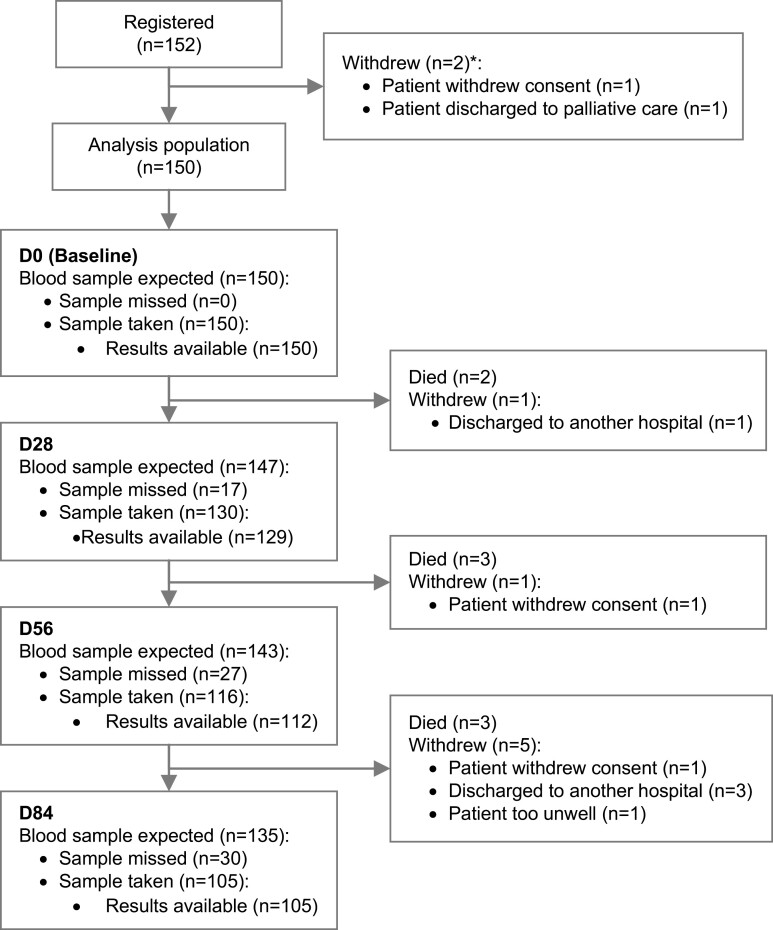
Materials and methods: Between September 2020 and April 2021, patients with cancer undergoing chemotherapy were enrolled. At baseline (day 0), days 28, 56, and 84, we assessed serum antibodies to SARS-CoV-2 spike (anti-S) and anti-nucleocapsid (anti-NP) and concomitantly assessed virus neutralization using a pseudovirus neutralization assay. Patients received either the Pfizer/BioNTech BNT162b2, or the Oxford/AstraZeneca ChAdOx1 vaccine.
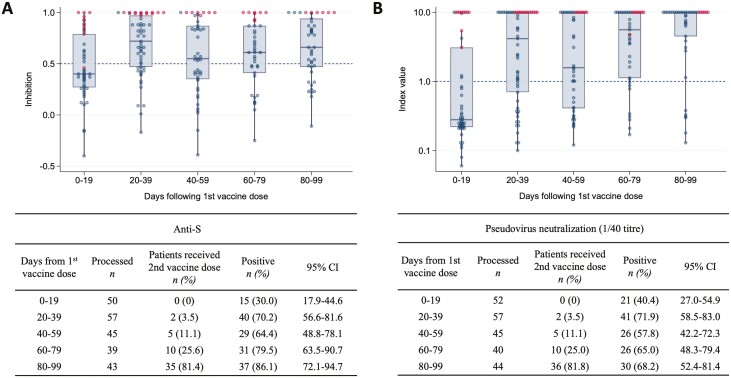
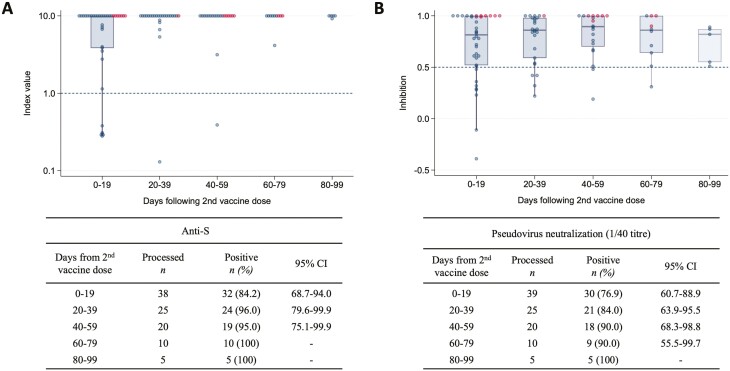
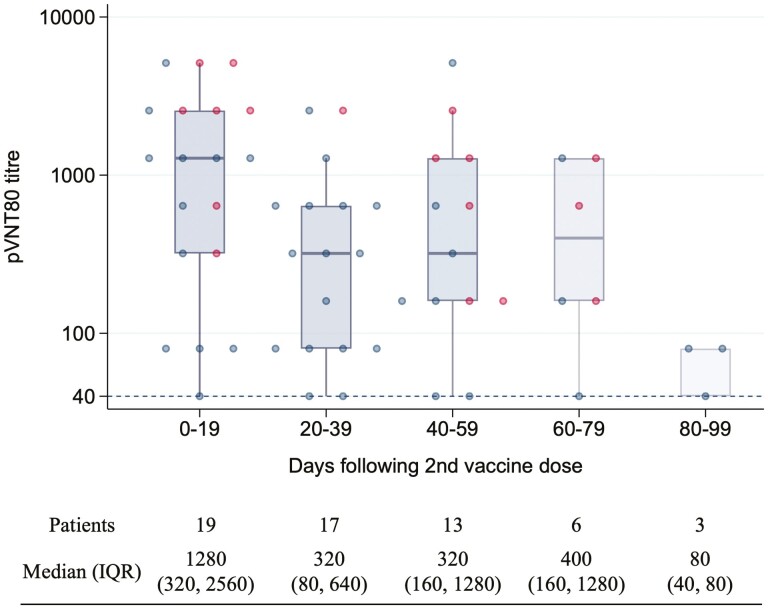
Results: All 152 patients enrolled had a prior diagnosis of cancer; colorectal (n = 80, 52.6%), oesophagogastric (n = 38, 25.0%), and hepato pancreatic biliary (n = 22, 12.5%). Nearly all were receiving systemic anti-cancer therapy (99.3%). Of the 51 patients who did not receive a vaccination prior to, or during the study, 5 patients had detectable anti-NP antibodies. Ninety-nine patients received at least one dose of vaccine prior to, or during the study. Within 19 days following the first dose of vaccine, 30.0% had anti-S detected in serum which increased to 70.2% at days 20-39. In the 19 days following a second dose, anti-S positivity was 84.2% (32/38). However, pseudovirus neutralization titers (pVNT80) decreased from days 20 to 39.
Conclusion: Despite the immunosuppressive effects of chemotherapy, 2 doses of SARS-CoV-2 vaccines are able to elicit a protective immune response in patients' ongoing treatment for gastrointestinal cancers. Decreases in pseudoviral neutralization were observed after 20-39 days, re-affirming the current recommendation for vaccine booster doses.
Clinical trial registration number: NCT04427280.
Keywords: COVID-19; SARS-CoV-2; anti-spike; chemotherapy; gastrointestinal cancer; immunity; pseudovirus; vaccines.
© The Author(s) 2022. Published by Oxford University Press.
Conflict of interest statement
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard. Accessed March 3, 2022. http://covid19.who.int
-
- Voysey M, Clemens SAC, Madhi SA, et al. Oxford COVID Vaccine Trial Group. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet (London, England). 2021;397(10269):99-111. 10.1016/S0140-6736(20)32661-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
