

Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition)
- PMID: 36342574
- PMCID: PMC9813208
- DOI: 10.1007/s10120-022-01331-8
Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition)
Abstract
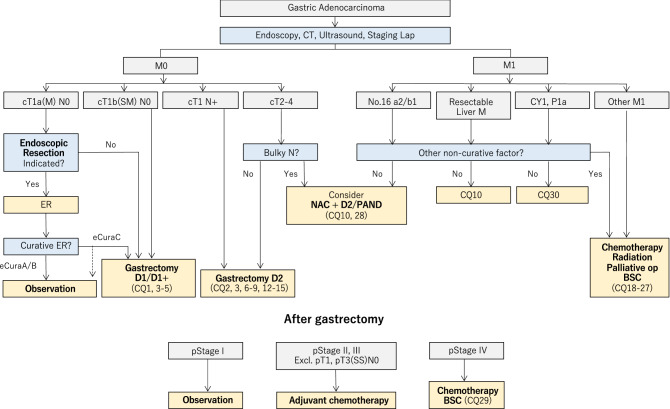
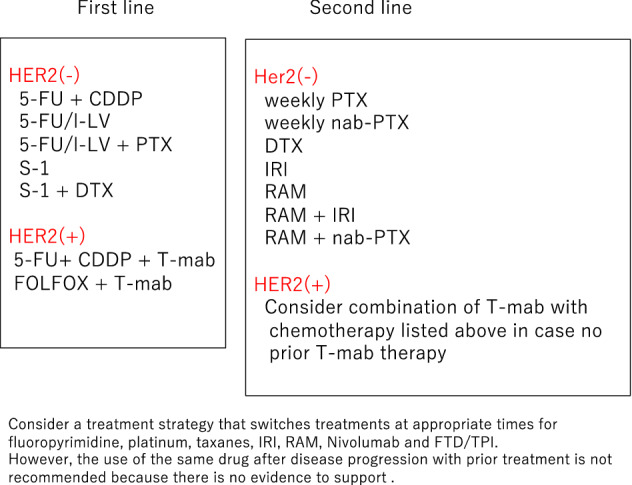
The sixth edition of the Japanese Gastric Cancer Treatment Guidelines was completed in July 2021, incorporating new evidence that emerged after publication of the previous edition. It consists of a text-based "Treatments" part and a "Clinical Questions" part including recommendations and explanations for clinical questions. The treatments parts include a comprehensive description regarding surgery, endoscopic resection and chemotherapy for gastric cancer. The clinical question part is based on the literature search and evaluation by an independent systematic review team. Consequently, not only evidence for each therapeutic recommendation was clearly shown, but it also identified the research fields that require further evaluation to provide appropriate recommendations.
Keywords: Chemotherapy; Endoscopic resection; Evidence based; Surgery; Treatment guidelines.
© 2022. The Author(s).
Conflict of interest statement
Dr. Baba reports research grants from Chugai, Eli Lilly, and Taiho, a speaker honorarium from Chugai, Eli Lilly, Taiho, Ono, MSD, Merck, Dai-ichi Sankyo, Tsumura, Miyarisan, Yakult, Eisai, Sanofi, BMS, Novartis, Janssen, and Takeda, and participation on a data safety monitoring board of Eli Lilly, Astellas, AstraZeneca, and Dai-ichi Sankyo outside the submitted work. Dr. Terashima reports a speaker honorarium from Taiho, Chugai, Ono, BMS, Yakult, Takeda, Eli Lilly, Pfizer, Dai-ichi Sankyo, Johnson and Johnson, Medtronic Japan, Intuitive Surgical Japan, and Olympus outside the submitted work. Dr. Fujishiro reports research grants from Olympus and Fujifilm, royalties from Hoya, a speaker honorarium from Olympus and Fujifilm, patents issued from Hoya, and an unpaid directorship of Japan Gastroenterological Endoscopy Society outside the submitted work.
Figures






References
-
- Association Japanese Gastric Cancer . Japanese Classification of Gastric Carcinoma. 15. Tokyo : Kanehara Shuppan; 2017.
-
- Brierley JD, Gospodarowicz MK, Wittekind C, editors. TNM classification of malignant tumours. 8. New Jersey: Wiley Blackwell; 2017.
-
- Terashima M, Fujitani K, Ando M, et al. Survival analysis of a prospective multicenter observational study on surgical palliation among patients receiving treatment for malignant gastric outlet obstruction caused by incurable advanced gastric cancer. Gastric Cancer. 2021;24:224–231. doi: 10.1007/s10120-020-01114-z. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
