

Discontinuation versus continuation of hypertonic saline or dornase alfa in modulator treated people with cystic fibrosis (SIMPLIFY): results from two parallel, multicentre, open-label, randomised, controlled, non-inferiority trials
- PMID: 36343646
- PMCID: PMC10065895
- DOI: 10.1016/S2213-2600(22)00434-9
Discontinuation versus continuation of hypertonic saline or dornase alfa in modulator treated people with cystic fibrosis (SIMPLIFY): results from two parallel, multicentre, open-label, randomised, controlled, non-inferiority trials
Abstract
Background: Reducing treatment burden is a priority for people with cystic fibrosis, whose health has benefited from using new modulators that substantially increase CFTR protein function. The SIMPLIFY study aimed to assess the effects of discontinuing nebulised hypertonic saline or dornase alfa in individuals using the CFTR modulator elexacaftor plus tezacaftor plus ivacaftor (ETI).
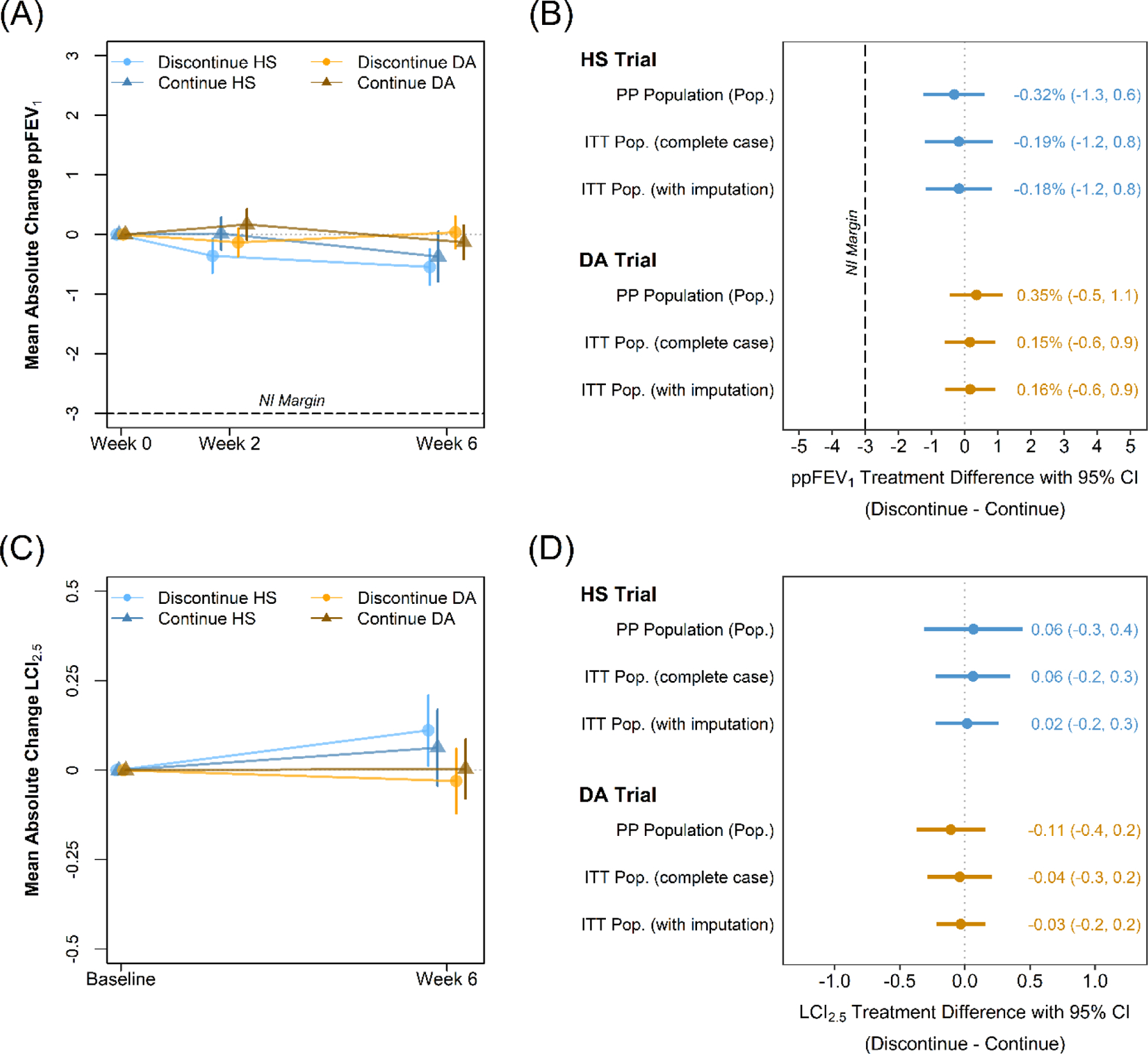
Methods: The SIMPLIFY study included two parallel, multicentre, open-label, randomised, controlled, non-inferiority trials at 80 participating clinics across the USA in the Cystic Fibrosis Therapeutics Development Network. We included individuals with cystic fibrosis aged 12-17 years with percent predicted FEV1 (ppFEV1) of 70% or more, or those aged 18 years or older with ppFEV1 of 60% or more, if they had been taking ETI and either (or both) mucoactive therapies (≥3% hypertonic saline or dornase alfa) for at least 90 days before screening. Participants on both hypertonic saline and dornase alfa were randomly assigned to one of the two trials, and those on a single therapy were assigned to the applicable trial. All participants were then randomly assigned 1:1 to continue or discontinue therapy for 6 weeks using permuted blocks of varying size, stratified by baseline ppFEV1 (week 0; ≥90% or <90%), single or concurrent use of hypertonic saline and dornase alfa, previous SIMPLIFY study participation (yes or no), and age (≥18 or <18 years). For participants randomly assigned to continue their therapy during a given trial, this therapy was instructed to be taken at least once daily according to each participant's pre-existing, clinically prescribed regimen. Hypertonic saline concentration was required to be at least 3%. The primary objective for each trial was to determine whether discontinuing was non-inferior to continuing, measured by the 6-week change in ppFEV1 in the per-protocol population. We established a non-inferiority margin of -3% for the difference between groups in the 6-week change in ppFEV1. Safety outcomes were analysed in the intention-to-treat population. This study is registered with ClinicalTrials.gov, NCT04378153.
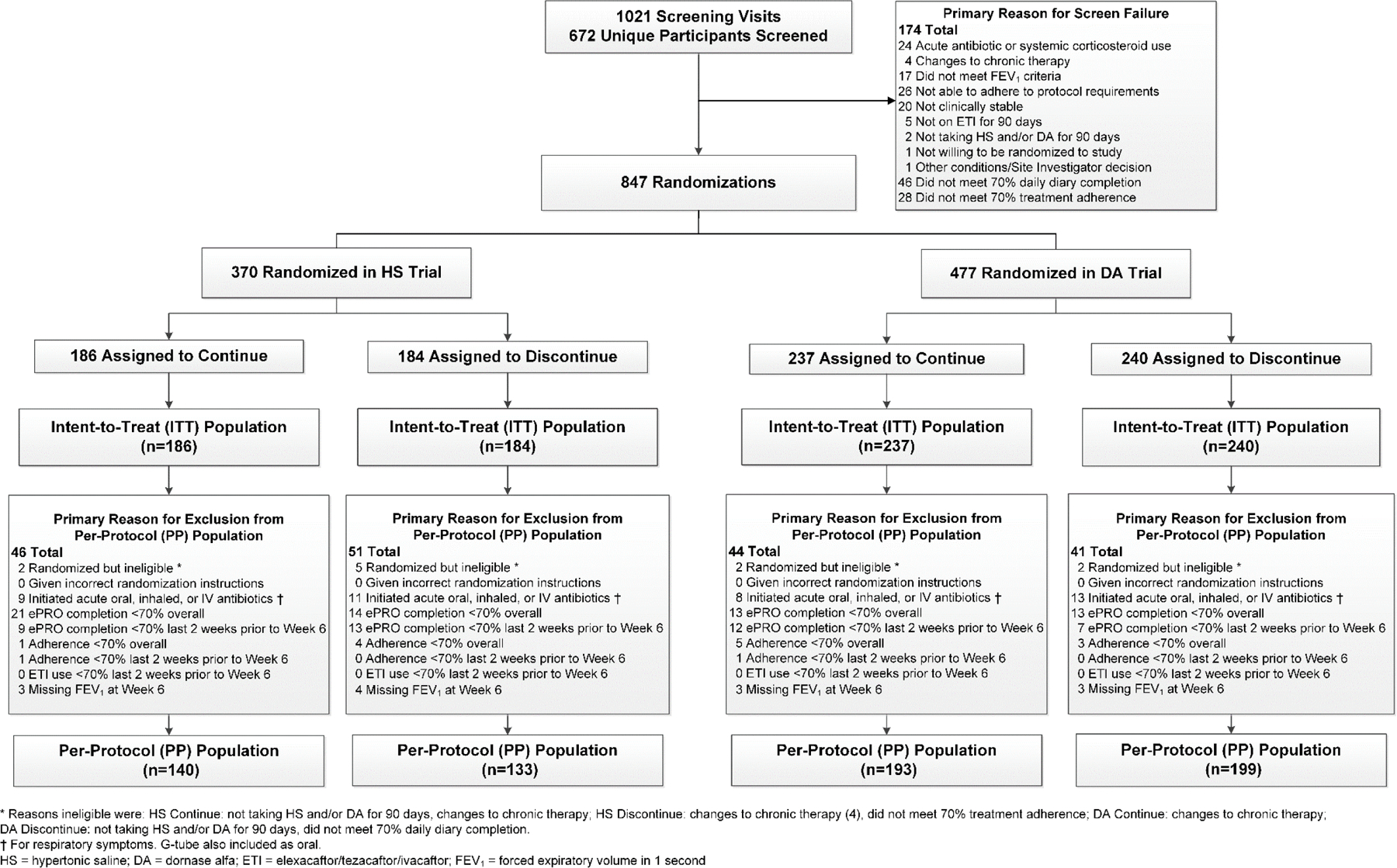
Findings: From Aug 25, 2020, to May 25, 2022, a total of 672 unique participants were screened for eligibility for one or both trials, resulting in 847 total random assignments across both trials with 594 unique participants. 370 participants were randomly assigned in the hypertonic saline trial and 477 in the dornase alfa trial. Participants across both trials had an average ppFEV1 of 96·9%. Discontinuing treatment was non-inferior to continuing treatment with respect to the absolute 6-week change in ppFEV1 in both the hypertonic saline trial (-0·19% [95% CI -0·85 to 0·48] in the discontinuation group [n=133] vs 0·14% [-0·51 to 0·78] in the continuation group [n=140]; between-group difference -0·32% [-1·25 to 0·60]) and dornase alfa trial (0·18% [-0·38 to 0·74] in the discontinuation group [n=199] vs -0·16% [-0·73 to 0·41] in the continuation group [n=193]; between-group difference 0·35% [-0·45 to 1·14]), with consistent results in the intention-to-treat populations. In the hypertonic saline trial, 64 (35%) of 184 in the discontinuation group versus 44 (24%) of 186 participants in the continuation group and, in the dornase alfa trial, 89 (37%) of 240 in the discontinuation group versus 55 (23%) of 237 in the continuation group had at least one adverse event.
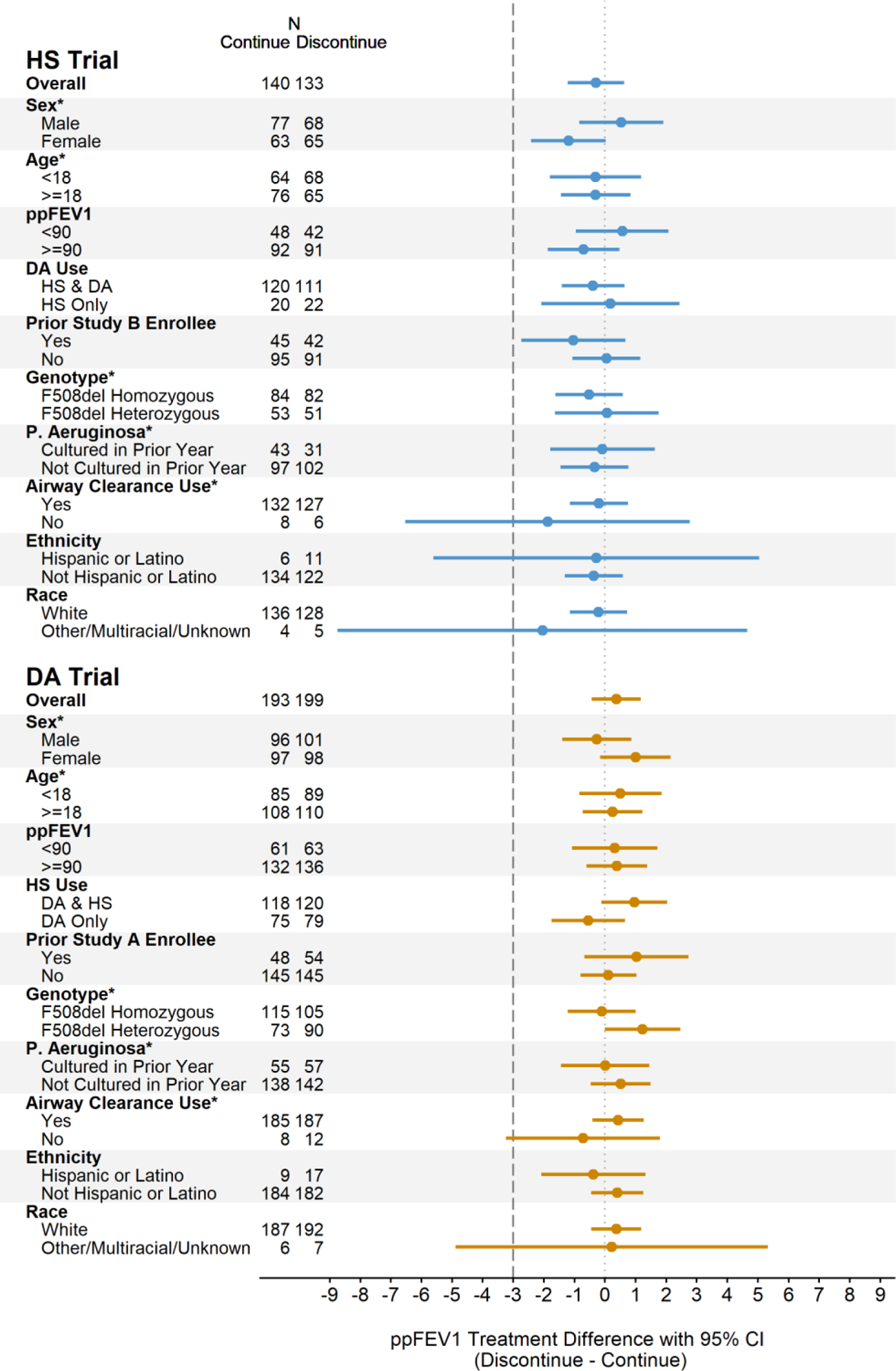
Interpretation: In individuals with cystic fibrosis on ETI with relatively well preserved pulmonary function, discontinuing daily hypertonic saline or dornase alfa for 6 weeks did not result in clinically meaningful differences in pulmonary function when compared with continuing treatment.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests GR-B reports grants and contracts from Vertex Pharmaceuticals and the Cystic Fibrosis Foundation (CFF). SHD reports contracts from AstraZeneca, Calithera, CFF, US National Institutes of Health (NIH), Vertex Pharmaceuticals; consulting fees from Polarean, 501 Ventures, and Chiesi USA; fees for advisory boards for Enterprise Therapeutics and Gilead Sciences; and participation on a data safety monitoring board (DSMB) for Abbvie and Boehringer Ingleheim. JLT-C reports grants and contracts from CFF, Vertex Pharmaceutics, Eloxx, and 4DMT; consulting fees from Vertex Phamaceuticals, Insmed, and 4DMT; participation on a DSMB for Abbvie; and serving on an advisory board for CFF, American Thoracic Society (ATS), Journal of Cystic Fibrosis, and Emily's Entourage. KAR reports grants from CFF; royalties from Springer Publishing; honoraria from Vertex Pharmaceuticals; and serving on an advisory board for ATS. AB reports grants from the CFF for Therapeutics Development Network (TDN) studies. FR reports grants from Vertex Phamaceuticals and consulting fees from Vertex Phamaceuticals, Proteostasis, Translate Bio, Boehringer Ingelheim, and Calithera. JKY reports grants from CFF. SM reports grants from CFF to support TDN studies. DPN reports grants from CFF and NIH; consulting fees from BiomX, Clarametyx, Genentech, GlaxoSmithKline, Nabriva, Respirion, and Vertex Pharmaceuticals; and advisory board membership for CFF and Kither Biotechnology. DR reports grants and contracts from CFF and Vertex Pharmaceuticals. AHG reports grants and contracts from CFF, Insmed, AbbVie, and 4D Molecular Therapeutics. GSS reports advisory board participation for Vertex Pharmaceuticals and Gilead Sciences. CHG reports grants and contracts from CFF, NIH, and the US Food and Drug Administration; consulting fees from Enterprise Therapeutics; and honoraria from Gilead Sciences, Novartis, Boehringer Ingelheim, Vertex Phamaceuticals, and stock options in Aer Therapeutics. JPC reports employment at the CFF. NM-H reports grants from CFF, NIH, and US Food and Drug Administration; consulting fees from Enterprise Therapeutics; and DSMB membership for the NIH. BPO, KO-D, AHG, GO, CA, RR, and KM declare no competing interests.
Figures
Comment in
-
SIMPLIFYing cystic fibrosis treatment in a post-modulator era.Lancet Respir Med. 2023 Apr;11(4):299-300. doi: 10.1016/S2213-2600(22)00480-5. Epub 2022 Dec 1. Lancet Respir Med. 2023. PMID: 36463912 No abstract available.
-
Reducing treatment burden in the era of CFTR modulators.Lancet Respir Med. 2023 Sep;11(9):e78. doi: 10.1016/S2213-2600(23)00223-0. Epub 2023 Jun 12. Lancet Respir Med. 2023. PMID: 37321239 No abstract available.
References
-
- Shteinberg M, Haq IJ, Polineni D, Davies JC. Cystic fibrosis. Lancet 2021; 397(10290): 2195–211. - PubMed
-
- Nichols DP, Chmiel JF. Inflammation and its genesis in cystic fibrosis. Pediatric pulmonology 2015; 50 Suppl 40: S39–56. - PubMed
-
- Ma JT, Tang C, Kang L, Voynow JA, Rubin BK. Cystic Fibrosis Sputum Rheology Correlates With Both Acute and Longitudinal Changes in Lung Function. Chest 2018; 154(2): 370–7. - PubMed
