

Hypofractionated, 3-week, preoperative radiotherapy for patients with soft tissue sarcomas (HYPORT-STS): a single-centre, open-label, single-arm, phase 2 trial
- PMID: 36343656
- PMCID: PMC9817485
- DOI: 10.1016/S1470-2045(22)00638-6
Hypofractionated, 3-week, preoperative radiotherapy for patients with soft tissue sarcomas (HYPORT-STS): a single-centre, open-label, single-arm, phase 2 trial
Abstract
Background: The standard preoperative radiotherapy regimen of 50 Gy delivered in 25 fractions for 5 weeks for soft tissue sarcomas results in excellent local control, with major wound complications occurring in approximately 35% of patients. We aimed to investigate the safety of a moderately hypofractionated, shorter regimen of radiotherapy, which could be more convenient for patients.
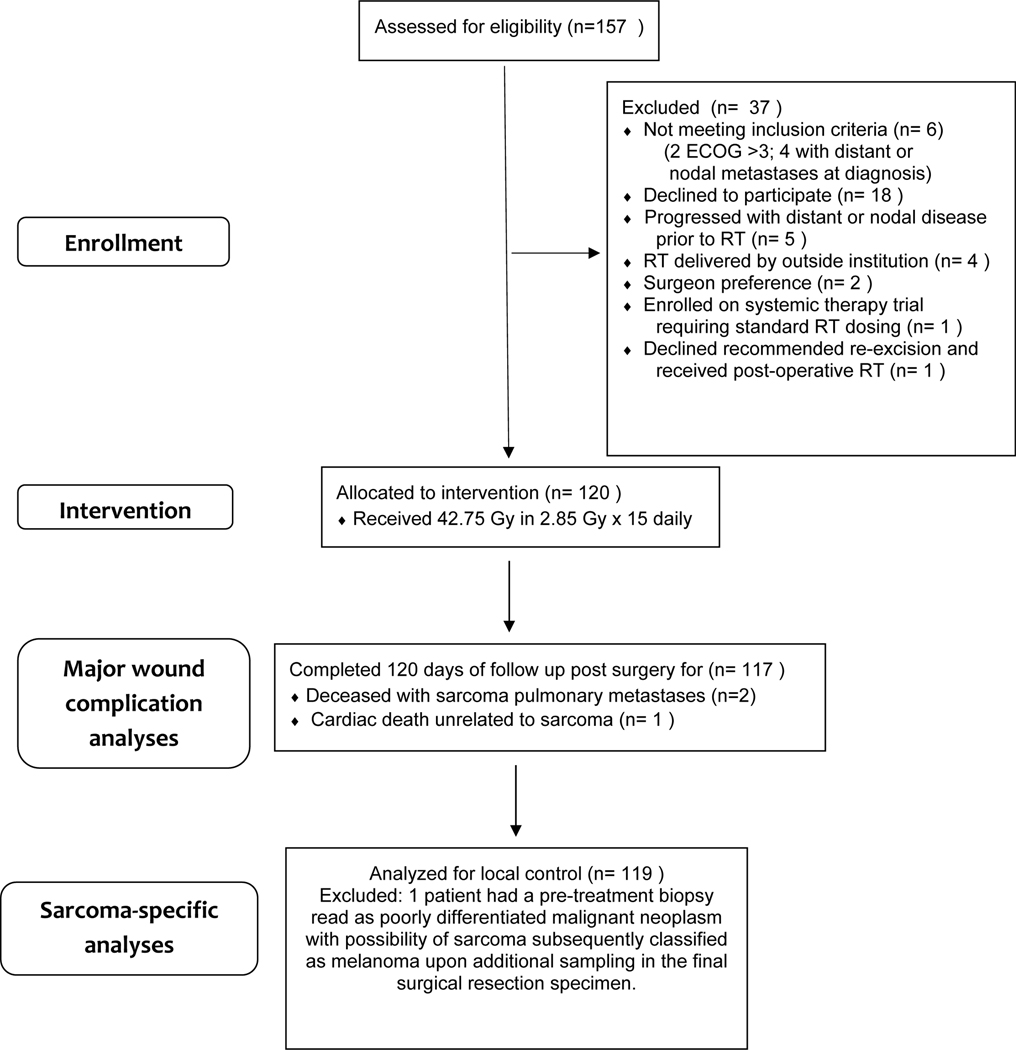
Methods: This single-centre, open-label, single-arm, phase 2 trial (HYPORT-STS) was done at a single tertiary cancer care centre (MD Anderson Cancer Center, Houston, TX, USA). We administered preoperative radiotherapy to a dose of 42·75 Gy in 15 fractions of 2·85 Gy/day for 3 weeks (five fractions per week) to adults (aged ≥18 years) with non-metastatic soft tissue sarcomas of the extremities or superficial trunk and an Eastern Cooperative Oncology Group performance status of 0-3. The primary endpoint was a major wound complication occurring within 120 days of surgery. Major wound complications were defined as those requiring a secondary operation, or operations, under general or regional anaesthesia for wound treatment; readmission to the hospital for wound care; invasive procedures for wound care; deep wound packing to an area of wound measuring at least 2 cm in length; prolonged dressing changes; repeat surgery for revision of a split thickness skin graft; or wet dressings for longer than 4 weeks. We analysed our primary outcome and safety in all patients who enrolled. We monitored safety using a Bayesian, one-arm, time-to-event stopping rule simulator comparing the rate of major wound complications at 120 days post-surgery among study participants with the historical rate of 35%. This trial is registered with ClinicalTrials.gov, NCT03819985, recruitment is complete, and follow-up continues.
Findings: Between Dec 18, 2018, and Jan 6, 2021, we assessed 157 patients for eligibility, of whom 120 were enrolled and received hypofractionated preoperative radiotherapy. At no time did the stopping rule computation indicate that the trial should be stopped early for lack of safety. Median postoperative follow-up was 24 months (IQR 17-30). Of 120 patients, 37 (31%, 95% CI 24-40) developed a major wound complication at a median time of 37 days (IQR 25-59) after surgery. No patient had acute radiation toxicity (during radiotherapy or within 4 weeks of the radiotherapy end date) of grade 3 or worse (Common Terminology Criteria for Adverse Events [CTCAE] version 4.0) or an on-treatment serious adverse event. Four (3%) of 115 patients had late radiation toxicity (≥6 months post-surgery) of at least grade 3 (CTCAE or Radiation Therapy Oncology Group/European Organisation for Research and Treatment of Cancer Late Radiation Morbidity Scoring Scheme): femur fractures (n=2), lymphoedema (n=1), and skin ulceration (n=1). There were no treatment-related deaths.
Interpretation: Moderately hypofractionated preoperative radiotherapy delivered to patients with soft tissue sarcomas was safe and could therefore be a more convenient alternative to conventionally fractionated radiotherapy. Patients can be counselled about these results and potentially offered this regimen, particularly if it facilitates care at a sarcoma specialty centre. Results on long-term oncological, late toxicity, and functional outcomes are awaited.
Funding: The National Cancer Institute.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests BAG reports grant support for research, for which she is co-principal investigator, to her institution from the Cancer Prevention and Research Institute of Texas (grant RP1606074) that is unrelated to this work. RR reports research funding to his institution from SpringWorks and C4 Therapeutics, consulting fees to his institution from Ayala Pharmaceuticals, and personal consulting fees and honoraria from Bayer and Epizyme. KET reports research funding to her institution from the US National Science Foundation and the Department of Defense and consulting fees to her personally from the US Department of Defense. KKH reports research funding to her institution from Cairn Surgical, Eli Lilly, and Lumicell, and is a medical advisory board member for Armada Health and AstraZeneca. RLS has received grant funding to his institution from the US Department of Defense for research unrelated to this report. JEB received personal consulting fees from GT Technologies. CLR reports research funding to her institution from Bristol Myers Squibb and personally received honoraria from Lumanity. All other authors declare no competing interests.
Figures
Comment in
-
Preoperative hypofractionated radiotherapy for soft tissue sarcoma.Lancet Oncol. 2022 Dec;23(12):1481-1482. doi: 10.1016/S1470-2045(22)00686-6. Lancet Oncol. 2022. PMID: 36455570 No abstract available.
-
Adopting shorter radiation regimens: rules of engagement for sarcoma.Lancet Oncol. 2023 Feb;24(2):e70. doi: 10.1016/S1470-2045(23)00008-6. Lancet Oncol. 2023. PMID: 36725150 Free PMC article. No abstract available.
References
-
- Yang JC, Chang AE, Baker AR, et al. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol Off J Am Soc Clin Oncol 1998; 16: 197–203. - PubMed
-
- O’Sullivan B, Davis AM, Turcotte R, et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet Lond Engl 2002; 359: 2235–41. - PubMed
-
- Cannon CP, Ballo MT, Zagars GK, et al. Complications of combined modality treatment of primary lower extremity soft-tissue sarcomas. Cancer 2006; 107: 2455–61. - PubMed
-
- Davis AM, Sennik S, Griffin AM, et al. Predictors of functional outcomes following limb salvage surgery for lower-extremity soft tissue sarcoma. J Surg Oncol 2000; 73: 206–11. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
