

High and low performers in internal rotation after reverse total shoulder arthroplasty: a biplane fluoroscopic study
- PMID: 36343789
- PMCID: PMC10023281
- DOI: 10.1016/j.jse.2022.10.009
High and low performers in internal rotation after reverse total shoulder arthroplasty: a biplane fluoroscopic study
Abstract
Background: Internal rotation in adduction is often limited after reverse total shoulder arthroplasty (rTSA), but the origins of this functional deficit are unclear. Few studies have directly compared individuals who can and cannot perform internal rotation in adduction. Little data on underlying 3D humerothoracic, scapulothoracic, and glenohumeral joint relationships in these patients are available.
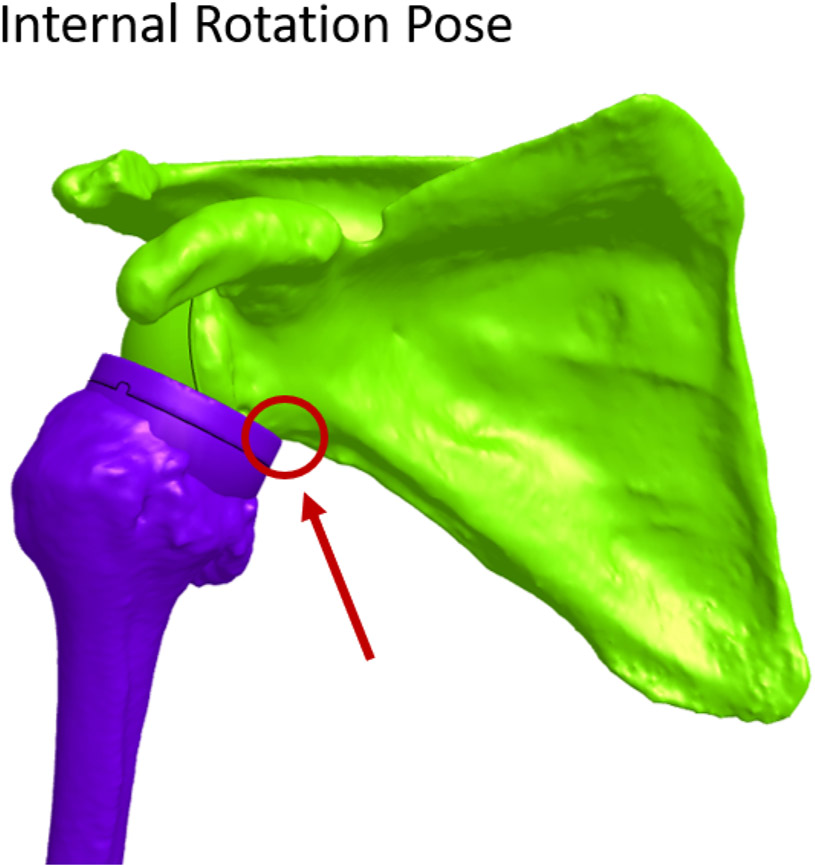
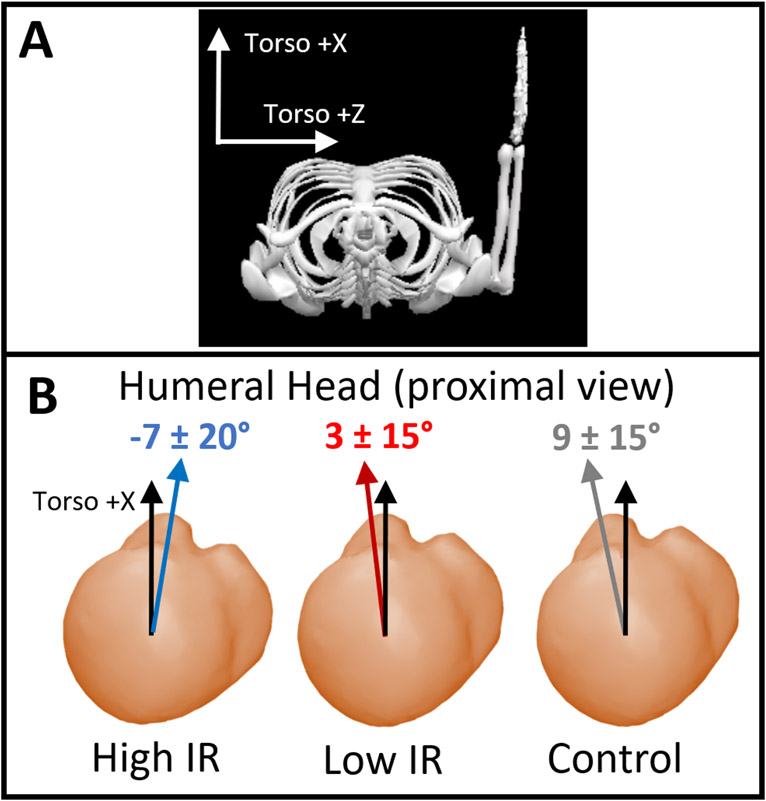
Methods: Individuals >1-year postoperative to rTSA were imaged with biplane fluoroscopy in resting neutral and internal rotation in adduction poses. Subjects could either perform internal rotation in adduction with their hand at T12 or higher (high, N = 7), or below the hip pocket (low, N = 8). Demographics, the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and scapular notching grade were recorded. Joint orientation angles were derived from model-based markerless tracking of the scapula and humerus relative to the torso. The 3D implant models were aligned to preoperative computed tomography models to evaluate bone-implant impingement.
Results: The Simple Shoulder Test was highest in the high group (11 ± 1 vs. 9 ± 2, P = .019). Two subjects per group had scapular notching (grades 1 and 2), and 3 high group and 4 low group subjects had impingement below the glenoid. In the neutral pose, the scapula had 7° more upward rotation in the high group (P = .100), and the low group demonstrated 9° more posterior tilt (P = .017) and 14° more glenohumeral elevation (P = .047). In the internal rotation pose, axial rotation was >45° higher in the high group (P ≤ .008) and the low group again had 11° more glenohumeral elevation (P = .058). Large rotational differences within subject groups arose from a combination of differences in the resting neutral and maximum internal rotation in adduction poses, not only the terminal arm position.
Conclusions: Individuals who were able to perform high internal rotation in adduction after rTSA demonstrated differences in joint orientation and anatomic biases versus patients with low internal rotation. The high rotation group had 7° more resting scapular upward rotation and used a 15°-30° change in scapular tilt to perform internal rotation in adduction versus patients in the low group. The combination of altered resting scapular posture and restricted scapulothoracic range of motion could prohibit glenohumeral rotation required to reach internal rotation in adduction. In addition, inter-patient variation in humeral torsion may contribute substantially to postoperative internal rotation differences. These data point toward modifiable implant design and placement factors, as well as foci for physical therapy to strengthen and mobilize the scapula and glenohumeral joint in response to rTSA surgery.
Keywords: Anatomic bias; Internal rotation; Joint angles; Reverse total shoulder arthroplasty; Shoulder.
Copyright © 2022 Journal of Shoulder and Elbow Surgery Board of Trustees. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: Peter Chalmers is a paid consultant for Depuy and DJO, receives intellectual property royalties from Depuy and Responsive Arthroscopy, receives research funding from Major League Baseball and LS Peery, and serves on the editorial board for the
Figures






References
-
- Barnes CJ, Van Steyn SJ, Fischer RA. The effects of age, sex, and shoulder dominance on range of motion of the shoulder. J Shoulder Elbow Surg 2001;10:242–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
