

Compartmentalization of the host microbiome: how tumor microbiota shapes checkpoint immunotherapy outcome and offers therapeutic prospects
- PMID: 36343977
- PMCID: PMC9644363
- DOI: 10.1136/jitc-2022-005401
Compartmentalization of the host microbiome: how tumor microbiota shapes checkpoint immunotherapy outcome and offers therapeutic prospects
Abstract
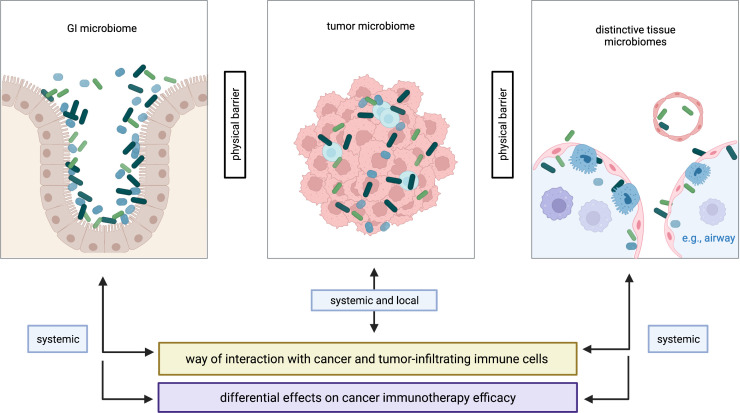
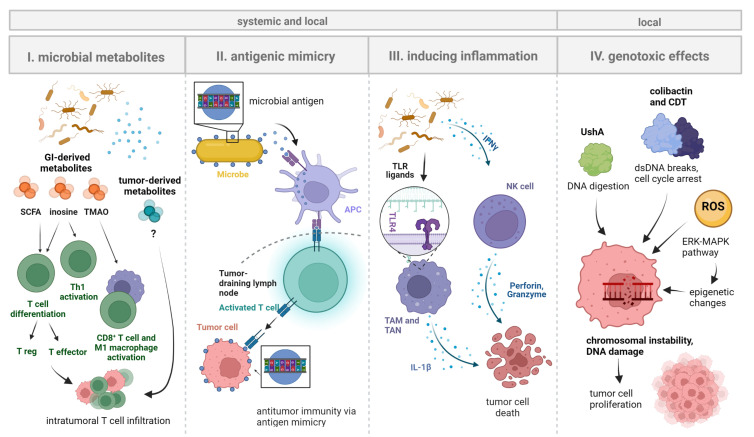
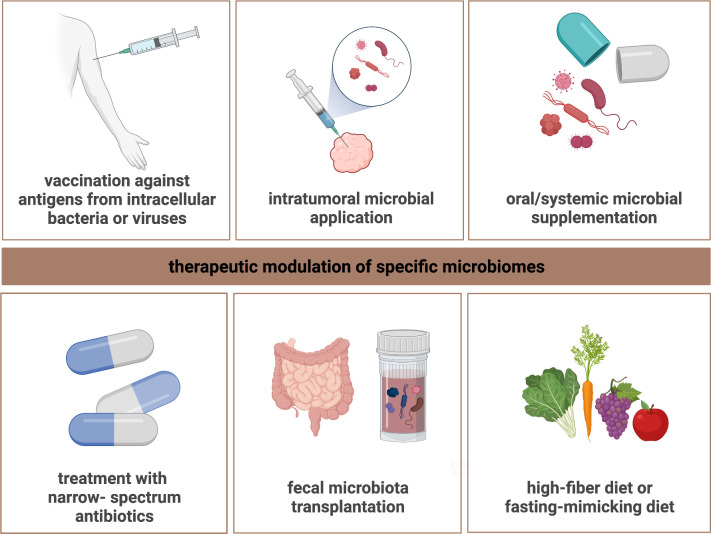
The host microbiome is polymorphic, compartmentalized, and composed of distinctive tissue microbiomes. While research in the field of cancer immunotherapy has provided an improved understanding of the interaction with the gastrointestinal microbiome, the significance of the tumor-associated microbiome has only recently been grasped. This article provides a state-of-the-art review about the tumor-associated microbiome and sheds light on how local tumor microbiota shapes anticancer immunity and influences checkpoint immunotherapy outcome. The direct route of interaction between cancer cells, immune cells, and microbiota in the tumor microenvironment is emphasized and advocates a focus on the tumor-associated microbiome in addition to the spatially separated gut compartment. Since the mechanisms underlying checkpoint immunotherapy modulation by tumor-associated microbiota remain largely elusive, future research should dissect the pathways involved and outline strategies to therapeutically modulate microbes and their products within the tumor microenvironment. A more detailed knowledge about the mechanisms governing the composition and functional quality of the tumor microbiome will improve cancer immunotherapy and advance precision medicine for solid tumors.
Keywords: Immunotherapy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MB serves as an advisor for Pantec Biosolutions AG. The other authors have no potential conflicts of interest to declare. No medical writer was involved in the preparation of the manuscript.
Figures
References
-
- Motzer RJ, Rini BI, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol 2019;20:1370–85. 10.1016/S1470-2045(19)30413-9 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical